Questions:
11. When is treatment indicated for carotid-cavernous fistulas?
12. What are the findings of thrombosis of the cavernous sinus?
13. What is the usual cause of cavernous sinus thrombosis?
14. What should be considered in a patient with apparent orbital cellulitis?
15. What are the major risks of thrombosis of the cavernous sinus?
16. What are 3 very serious complications of cavernous sinus thrombosis?
17. What is the mnemonic for the structures and their position in the cavernous sinus?
18. What is the cause of “orbital varices”?
19. What should be considered when a crying infant eye bulges?
____________________________________________________
Questions with answers:
11. When is treatment indicated for carotid-cavernous fistulas?
Treatment is indicated in all cases of direct carotid fistula and for indirect fistulas with visual loss or cortical vein drainage which has a high risk of intracranial hemorrhage.
12. What are the findings of thrombosis of the cavernous sinus?
1. An acute or subacute orbital syndrome
2. Pain (periorbital and headache)
3. Proptosis with periorbital edema (often periorbital ecchymoses)
4. Chemosis
5. Visual loss (optic neuropathy, venous congestion with disk edema and retinal hemorrhages),
6. Increased intraocular pressure
7. Ophthalmoplegia (multiple cranial nerve palsies, and enlargement of extraocular muscles from venous congestion)
8. Systemic symptoms (fever and altered mental status)
13. What is the usual cause of cavernous sinus thrombosis?
A severe facial, sinus, or orbital infection. It is rarely secondary to a hypercoagulable state.
14. What should be considered in a patient with apparent orbital cellulitis?
Cavernous sinus thrombosis, a serious complication of paranasal sinusitis that most commonly results from the anterograde spread of infection involving the mid-third of the face (e.g., orbit, mouth, paranasal sinuses), may be difficult to distinguish from simple orbital cellulitis. It may also occur with and be caused by orbital cellulitis.
15. What are the major risks of thrombosis of the cavernous sinus?
There is a high rate of morbidity and mortality with a risk of extension of the venous thrombosis to intracranial veins and cerebral infarction, as well as a high risk of permanent visual loss.
16. What are 3 very serious complications of cavernous sinus thrombosis?
1. Cerebral abscess
2. Infectious meningitis
3. Spread of infection to the contralateral cavernous sinus and fellow orbit.
17. What is the mnemonic for the structures and their position in the cavernous sinus?
O TOM CAT
– OTOM is for the items going down the lateral wall (O: Oculomotor nerve, T: Trochlear nerve, O: ophthalmic branch of the trigeminal nerve, M: Maxillary branch of the trigeminal nerve)
– CAT from medial to lateral (C: Internal carotid artery, A: Abducens nerve, T: Trochlear nerve)
18. What is the cause of “orbital varices”?
Venous angiomas may occur in the orbit and are often called orbital varices. Clinical presentation is characteristic and results from intermittent filling and emptying of the varix, resulting in variable proptosis.
19. What should be considered when a crying infant eye bulges?
Consider orbital varix (venous angioma) when an eye bulges in a crying infant, there is proptosis during Valsalva maneuver or orbital ecchymoses.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
15.4 Carotid-Cavernous Thrombosis
15.4.1 Features and Causes
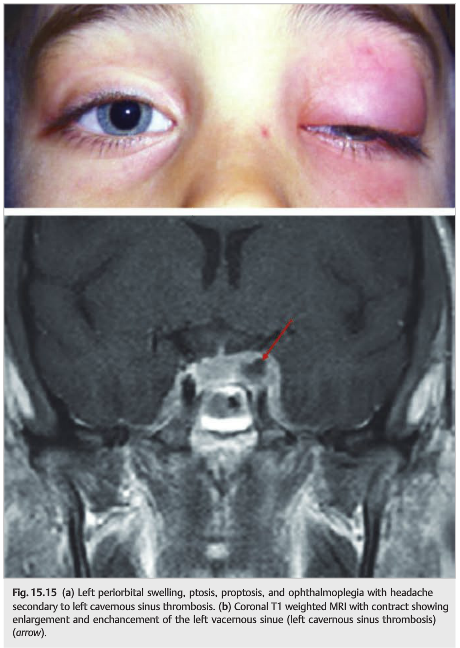
Thrombosis of the cavernous sinus produces an acute or subacute orbital syndrome(▶Fig. 15.15), which includes the following:
● Pain (periorbital and headache)
● Proptosis with periorbital edema (often periorbital ecchymoses)
● Chemosis
● Visual loss
○ Optic neuropathy
○ Venous congestion with disc edema and retinal hemorrhages○ Increased intraocular pressure
● Ophthalmoplegia○ Multiple cranial nerve palsies in the cavernous sinus○ Enlargement of extraocular muscles from venous congestion
● Systemic symptoms such as fever and altered mental status
Cavernous sinus thrombosis is usually a complication of a severe facial, sinus, or orbital infection. It is rarely secondary to a hypercoagulable state.
15.4.2 Prognosis and Treatment
There is a high rate of morbidity and mortality with risk of extension of the venous thrombosis to intracranial veins and cerebral infarction, as well as a high risk of permanent visual loss. The prognosis is mostly based on the cause of the cavernous sinus thrombosis: severe facial and sinus infections can be complicated by cerebral abscess, infectious meningitis, and spread of infection to the contralateral cavernous sinus and fellow orbit. Treatment includes aggressive treatment of the underlying cause. If there is local infection, treatment would include drainage and administration of antibiotics, as well as anticoagulation therapy. Corticosteroids are sometimes started once the infection is controlled to reduce inflammation and edema.
15.5 Superior Ophthalmic Vein Thrombosis

Thrombosis is of the orbital veins produces a very acute and severe orbital syndrome (▶Fig. 15.16). It is rare and usually occurs in the setting of sepsis or hypercoagulable state. It may also complicate a cavernous sinus thrombosis or a CCF.
15.6 Orbital Varix

Venous angiomas may occur in the orbit and are usually called orbital varices (▶Fig. 15.17). Clinical presentation is characteristic and results from intermittent filling and emptying of the varix, resulting in variable proptosis.
Pearls
Consider orbital varix when there is eye bulging in a crying infant, proptosis during Valsalva maneuver, or orbital ecchymoses.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.