Questions:
1. What symptoms and signs may develop from an aneurysm of the internal carotid artery within the cavernous sinus?
2. What are the characteristics of direct shunts between the internal carotid artery and the cavernous sinus?
3. What are the characteristics of indirect carotid-cavernous or dural shunts?
4. Does a carotid-cavernous fistula have unilateral or bilateral ocular symptoms?
5. Do carotid-cavernous fistulas always have ocular symptoms?
6. What are 10 ocular findings of a carotid-cavernous fistula?
7. Which of the cranial nerves is most commonly affected by a carotid-cavernous fistula?
8. Can mechanical restriction of extraocular muscles occur with a carotid-cavernous fistula?
9. What diagnosis should be considered in an elderly woman with a mild headache, and elevated intraocular pressure?
10. What should be considered in all patients with a bruit accompanying a chronically red eye?
____________________________________________________
Questions with answers:
1. What symptoms and signs may develop from an aneurysm of the internal carotid artery within the cavernous sinus?
Patients are often asymptomatic until they develop:
1. Diplopia (ocular motor nerve compression)
2. Ipsilateral pain (trigeminal nerve compression)
3. Ipsilateral third-order Horner syndrome.
There is usually no visual loss.
2. What are the characteristics of direct shunts between the internal carotid artery and the cavernous sinus?
1. 70 to 90% of all CCFs are direct
2. Usually have high-flow
3. Most often are post-traumatic or they can arise from rupture of an intracavernous carotid artery aneurysm or from complications of surgery or catheter angiography.
4. Usually are acute and with severe symptoms
5. Rarely resolve spontaneously.
3. What are the characteristics of indirect carotid-cavernous or dural shunts?
1. They are often congenital arteriovenous connections between small arterial branches and the cavernous sinus.
2. They open spontaneously in older women or in the setting of hypertension, diabetes, atherosclerotic disease, childbirth, or collagen-vascular disease.
3. They cause insidious and less severe symptoms.
4. They are much more likely than direct shunts to be misdiagnosed initially,
5. They are more likely to resolve spontaneously.
4. Does a carotid-cavernous fistula have unilateral or bilateral ocular symptoms?
Ocular manifestations are usually unilateral and ipsilateral to the fistula, but they may be bilateral or even contralateral because of the connections between the two cavernous sinuses.
5. Do carotid-cavernous fistulas always have ocular symptoms?
No, when arterial blood flow escapes posteriorly from the cavernous sinus through the petrosal sinuses, patients may not develop ocular symptoms or signs. When arterial blood flows anteriorly into the superior and/or inferior ophthalmic veins, ocular manifestations occur.
6. What are 10 ocular findings of a carotid-cavernous fistula?
1. Arterialization of the conjunctival vessels and chemosis
2. Proptosis
3. Elevated intraocular pressure resulting from increased episcleral venous pressure and orbital congestion, and rarely from neovascularization associated with chronic hypoxia or angle-closure glaucoma
4. Cranial or orbital bruit
5. Ophthalmoplegia
6. Ipsilateral optic disk swelling
7. Dilation of retinal veins
8. Intraretinal hemorrhages, preretinal or vitreous hemorrhages
9. Choroidal thickening/detachment
10. Retinal serous detachment.
7. Which of the cranial nerves is most commonly affected by a carotid-cavernous fistula?
The sixth cranial nerve
8. Can mechanical restriction of extraocular muscles occur with a carotid-cavernous fistula?
Yes, mechanical restriction of the extraocular muscles can result from venous stasis, orbital edema, and engorgement of the muscles.
9. What diagnosis should be considered in an elderly woman with a mild headache, and elevated intraocular pressure?
Carotid-cavernous fistula
10. What should be considered in all patients with a bruit accompanying a chronically red eye?
Carotid-cavernous fistula
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
15 Cavernous Sinus and Orbital Vascular Disorders
Cavernous sinus and orbital vascular disorders are commonly seen in neuro-ophthalmology. They include cavernous sinus aneurysms, carotid-cavernous fistulas, cavernous sinus thrombosis, and venous disorders of the orbit.
15.1 Vascular Drainage of the Orbit and Cavernous Sinus
Each cavernous sinus contains a plexus of veins draining the orbits and some of the intracranial veins (▶Fig. 15.1).
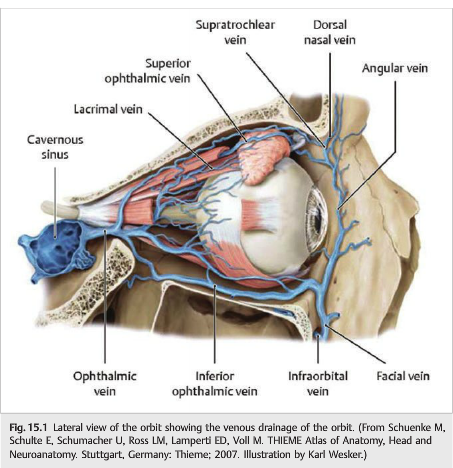
The carotid artery passes through the cavernous sinus. Vascular disorders are a common cause of cavernous sinus and orbital syndromes. The major orbital veins include the superior and the inferior ophthalmic veins. The cavernous sinus is connected anteriorly to the superior and inferior ophthalmic veins and posteriorly to the superior and inferior petrosal sinuses (▶Fig. 15.2).

There are numerous communications between the facial veins and the orbital veins, explaining why facial infections are often complicated by orbital cellulitis and rarely by cavernous sinus thrombosis. Impaired venous drainage results in orbital congestion, which presents like an orbital syndrome.
15.2 Carotid-Cavernous Aneurysms
Aneurysms of the internal carotid artery may develop within the cavernous sinus (▶Fig. 15.3 and ▶Fig. 15.4).


They are often asymptomatic until patients develop diplopia (ocular motor nerve compression) and ipsilateral pain (trigeminal nerve compression).An ipsilateral third-order Horner syndrome may be present. There is usually no visual loss.
15.3 Carotid-Cavernous Fistulas
A carotid-cavernous fistula (CCF) is an abnormal communication between the carotid artery and the cavernous sinus, a venous plexus (▶Fig. 15.5).

The cavernous sinus fills with arterial blood, and the pressure increases. This results in impaired drainage of all veins normally draining into the cavernous sinus with resultant venous congestion (▶Fig. 15.6).

15.3.1 Classification
CCFs can be classified by four different schemes:
1. Etiologically (traumatic or spontaneous)
2. Hemodynamically (high flow or low flow)
3. Anatomically (direct or dural)
4. Angiographically:
● Type A fistulas are direct shunts between the internal carotid artery and the cavernous sinus. They represent from 70 to 90% of all CCFs, are usually of the high-flow type, and most often are post traumatic. They can also arise from rupture of an intracavernous carotid artery aneurysm or from complications of surgery or catheter angiography. Because of the high blood flow rate, direct CCFs usually manifest with acute and severe symptoms, and they rarely resolve spontaneously.
● Types B, C, and D are indirect or dural shunts. They represent congenital arteriovenous connections between small arterial branches and the cavernous sinus that open spontaneously in older women or in the setting of hypertension, diabetes, atherosclerotic disease, childbirth, or collagen-vascular disease. Dural CCFs usually cause insidious and less severe symptoms. In contrast to direct fistulas, dural shunts are much more likely to be misdiagnosed initially and to resolve spontaneously.
15.3.2 Features
As a result of these abnormal communications between arteries and veins, and because of the baseline pressure gradient between the two, the affected veins become “arterialized,” with a resultant elevation in intravenous pressure and changes in the hemodynamics of the involved vasculature, including rate and direction of blood flow (▶Fig. 15.7, ▶Fig. 15.8, and ▶Fig. 15.9).


When arterial blood flow escapes posteriorly from the cavernous sinus through the petrosal sinuses, patients may not develop ocular symptoms or signs.
When arterial blood flows anteriorly into the superior and/or inferior ophthalmic veins, ocular manifestations occur from venous and arterial stasis within the eye and the orbit, increased episcleral venous pressure, and decreased arterial blood flow to the cranial nerves within the cavernous sinus. These manifestations are usually unilateral and ipsilateral to the fistula, but they may be bilateral or even contralateral because of the connections between the two cavernous sinuses.
Classic features in CCF include the following:
● Arterialization of the conjunctival vessels and conjunctival chemosis are a direct consequence of arterial blood flow into the orbital and conjunctival veins.
● Proptosis, from congestion of orbital tissues, is often one of the earliest findings. It is highly variable, commonly associated with eyelid swelling, and may produce exposure keratopathy.
● Elevated intraocular pressure results from increased episcleral venous pressure and orbital congestion, and rarely from neovascularization associated with chronic hypoxia or from angle closure glaucoma.
● There is usually a subjective or objective cranial bruit (detected by placing the bell of the stethoscope over the patient’s temple or the orbit). The bruit can sometimes be heard without a stethoscope.
● Ophthalmoplegia is common in CCFs and results from direct damage to the ocularmotor nerves by trauma (direct CCF), compression of the ocular motor nerves by a carotid-cavernous aneurysm, and the fistula itself causing ischemia and/or compression of the ocular motor nerves. The sixth cranial nerve is the most commonly affected nerve because of its free-floating location within the cavernous sinus. Mechanical restriction of the extraocular muscles results from venous stasis, orbital edema, and engorgement of the muscles.
Classic fundus findings in direct CCFs include the following (▶Fig. 15.10 and ▶Fig. 15.11):
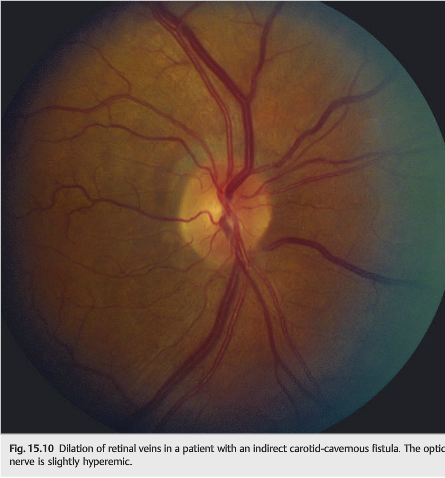

● Ipsilateral optic disc swelling
● Dilation of retinal veins
● Intraretinal hemorrhages from venous stasis and impaired retinal blood flow
● Preretinal or intravitreous hemorrhages (rare)
● Choroidal thickening, choroidal detachment, and retinal serous detachment
Pearls
Consider the diagnosis of CCF in all patients with elevated intraocular pressure, mild headache, or a bruit accompanying a chronically red eye, especially in elderly women.
The diagnosis of CCF is based on imaging (▶Fig. 15.12, ▶Fig. 15.13, and ▶Fig. 15.14).



Prominence of the superior ophthalmic vein and diffuse enlargement of all the extraocular muscles are frequently detected on computed tomographic (CT) scan or magnetic resonance imaging (MRI) or on orbital ultrasonography. Computed tomographic angiography (CTA) and magnetic resonance angiography (MRA) are not very useful, except for the source images. Definitive diagnosis depends on catheter angiographic evaluation, with selective injection of both internal and external carotid arteries and the vertebral circulation.
15.3.3 Prognosis
Visual loss associated with CCF may be immediate, most often from coincident ocular or optic nerve damage at the time of the head injury, or delayed, caused by exposure keratopathy, elevated intraocular pressure, vitreous hemorrhage, retinal venous stasis, central retinal vein occlusion, choroidal detachment, or anterior or posterior ischemic optic neuropathy. Although CCFs are rarely a life-threatening condition, patients with direct CCFs may have venous infarction, massive epistaxis, intracranial hemorrhage, or subarachnoid hemorrhage from rupture of the fistula.
15.3.4 Treatment
Treatment is indicated in all cases of direct carotid fistula and in indirect fistula with visual loss or cortical vein drainage (which have a high risk of intracranial hemorrhage).The ideal result is closure of the fistula and normalization of orbital hemodynamics, while preserving internal carotid artery patency. Occlusion of the fistula can be done by occlusion of the internal carotid artery (although there is a risk of ipsilateral cerebral infarction and ocular ischemic syndrome). Selective closure of the fistula without occlusion of the internal carotid artery can be done by endovascular approaches (embolization and detachable balloon occlusion) or, more rarely, by direct surgical approaches. Secondary glaucoma and ischemic retinopathy may require specific treatments.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.