Questions:
169. What is the Raymond syndrome?
170. What is the Millard-Gubler syndrome?
171. What is the Foville syndrome?
172. What is the Wallenberg syndrome?
173. What is the Weber syndrome?
174. What is the Nothnagel syndrome?
175. What is Benedikt syndrome?
176. What is the Claude syndrome?
177. What is the top of the basilar syndrome?
178. What is the Tolosa-Hunt syndrome?
_________________________________________
Questions with answers:
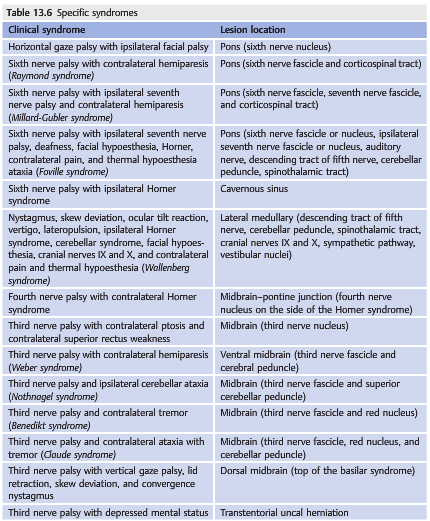
169. What is the Raymond syndrome?
6th nerve palsy with contralateral hemiparesis.
Lesion Location: Pons – ipsilateral 6th nerve fascicle and corticospinal tract
170. What is the Millard-Gubler syndrome?
6th nerve palsy with ipsilateral 7th nerve palsy and contralateral hemiparesis.
Lesion location: Pons – ipsilateral 6th nerve fascicle, 7th nerve fascicle, and corticospinal tract.
171. What is the Foville syndrome?
Ipsilateral 6th nerve palsy with ipsilateral 7th nerve palsy, deafness, hypoesthesia, Horner syndrome, contralateral pain and thermal hypoesthesia, ataxia.
Lesion location: Pons – 6th nerve fascicle or nucleus, ipsilateral 7th nerve fascicle or nucleus, auditory nerve, descending tract of 5th nerve, cerebellar peduncle, and spinothalamic tract.
172. What is the Wallenberg syndrome?
AKA Lateral medullary syndrome or posterior inferior cerebellar artery syndrome. The diagnostic finding is a loss of pain and temperature sensation on the contralateral side of the body and ipsilateral side of the face. Its findings include: nystagmus, skew deviation, ocular tilt reaction, vertigo, lateropulsion, ipsilateral 1st-order neuron Horner syndrome, cerebellar syndrome, facial hypoesthesia, cranial nerves IX and X, and contralateral pain and thermal hypoesthesia.
Lesion location: Lateral part of the medulla – descending tract of the 5th nerve, cerebellar peduncle, spinothalamic tract, cranial nerves IX and X, sympathetic pathway, and vestibular nuclei.
173. What is the Weber syndrome?
3rd nerve palsy with contralateral hemiparesis.
Lesion location: Ventral midbrain – 3rd nerve fascicle and cerebral peduncle.
174. What is the Nothnagel syndrome?
3rd nerve palsy and ipsilateral cerebellar ataxia.
Lesion location: Midbrain – 3rd nerve fascicle and cerebral peduncle.
175. What is Benedikt syndrome?
3rd nerve palsy and contralateral tremor.
Lesion location: Midbrain – 3rd nerve fascicle and red nucleus.
176. What is the Claude syndrome?
3rd nerve palsy and contralateral ataxia with tremor.
Lesion location: Midbrain – 3rd nerve fascicle, red nucleus, and cerebellar peduncle.
177. What is the top of the basilar syndrome?
3rd nerve palsy with vertical gaze palsy, lid retraction, skew deviation, and convergence nystagmus.
Lesion location: Dorsal midbrain.
178. What is the Tolosa-Hunt syndrome?
A painful ophthalmoplegia caused by nonspecific inflammation of the cavernous sinus or superior orbital fissure.
_________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
13.7 NOI13 Diplopia 11 – Vertical Eye Movements
Associated neurologic symptoms and signs localize the diplopia to the brainstem. Specific syndromes need to be known because of their highly localizing value (▶Table 13.6).
13.8 Treatment of Diplopia
Binocular diplopia resolves when the patient closes one eye. Most patients realize this spontaneously and patch one eye to suppress diplopia. This is an acceptable temporary treatment, either until the diplopia resolves by itself or until other treatments are decided on.
Many simple, common sense measures can improve the vision of diplopic patients.
For example, if a patient complains of diplopia only when looking down, then avoiding looking down may be the best treatment. This can be accomplished by recommending correction of presbyopia with single-vision reading glasses instead of bifocal or progressive lenses (which require that the patient look down to read); patients can also be advised to read sitting up with the book on a table or on a book (or music) stand instead of reading lying down in bed.
13.8.1 Patching
Any patch works. A nonsticky, removable patch is more comfortable. Many patients prefer semiopaque tape placed over one lens (on their regular glasses or on sunglasses). It suppresses diplopia as well as an opaque patch but still allows them to see shadows and use their peripheral vision while ambulating (▶Fig. 13.140).

In adults, patching one eye, even for a long period of time, does not alter visual function. Alternating the patch is not necessary, and patients can choose which eye to patch (they usually prefer not to patch the dominant eye or the eye that sees or moves best).
In young children (<10 years old), prolonged patching may induce amblyopia. This is why it is usually recommended to alternate patching in children.
Patching is usually the best acute solution for sick patients, patients in the hospital or in rehabilitation, and older patients who are at risk of falling.
13.8.2 Prisms
Diplopia can be corrected by placing a prism of appropriate power in front of one eye (the power of the prism is equivalent to the amount of ocular deviation measured with prisms).
This is usually a very good way to correct diplopia as long as the ocular deviation is not too large (usually<20 or 30 prism diopters) and is relatively stable (prisms are not a good solution for myasthenic patients whose diplopia fluctuates during the day).
Prisms are either temporary (Fresnel prisms are thin, soft plastic sheets than can be taped to the patient’s glasses and are easily removed) or permanent (prisms are ground invisibly into permanent glasses). Permanent prisms can be expensive and should be prescribed only when the diplopia has been stable for several months.
Prisms are not perfect because they correct incomitant diplopia in only one direction of gaze and because they degrade visual acuity and can induce distortion. They may not be tolerated in older patients with difficulty walking and with balance disorders.
13.8.3 Strabismus Surgery
Surgery on one or more extraocular muscles is a very effective way to definitively correct ocular misalignment. Surgery is performed only for relatively large deviations once they have been documented to be stable (it is usually recommended to wait at least 6 months after an injury resulting in diplopia before performing strabismus surgery). Surgery is highly successful for simple ocular deviations such as from a sixth nerve palsy or superior oblique paresis. It can be more difficult after a third nerve palsy.
13.8.4 Botulinum Toxin Injection
Injection of botulinum toxin into an extraocular muscle results in temporary (several weeks) paralysis of the muscle. This technique is used to temporarily straighten an eye in rare cases of severe ocular deviation from paralysis of a rectus muscle (e.g., some patients with trauma and a sixth nerve palsy may have a severe deviation of the affected eye toward the nose; injection of botulinum toxin in the medial rectus will weaken the medial rectus, and the eye will straighten for several weeks while recovering its normal function).
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.