Questions:
143. What are 7 characteristics of Skew Deviation?
144. What test can help differentiate a 4th nerve palsy from skew deviation?
145. What is the ocular tilt reaction?
146. What transmission pathway is disrupted in skew deviation and the ocular tilt reaction?
147. What infectious condition can cause a vertical gaze palsy?
148. What is the cause of Whipple disease?
149. What are the findings of Whipple disease?
150. Where are saccadic eye movements initiated?
151. Where are smooth pursuit eye movements generated?
152. What is the function of inputs to the visual system from the vestibular nuclear complexes?
153. What is Ocular Neuromyotonia?
154. What are the symptoms of Ocular Neuromyotonia?
155. What is the usual cause of Ocular Neuromyotonia?
____________________________________________________
Questions with answers:
143. What are 7 characteristics of Skew Deviation?
1. Skew deviation is an acquired vertical misalignment of the eyes resulting from asymmetric disruption of supranuclear input from the otolithic organs.
2. It commonly results from acute brainstem/cerebellar dysfunction.
3. Patients complain of vertical diplopia, sometimes with a torsional component (an exception to the general rule that supranuclear lesions do not produce diplopia).
4. There are usually other neurologic symptoms (e.g. ataxia).
5. The hypertropia of a skew deviation may be comitant or noncomitant.
6. When a skew deviation is noncomitant, it may be difficult to distinguish from a third nerve palsy or fourth nerve palsy.
7. Ocular torsion and head tilt may accompany a skew deviation (ocular tilt reaction).
144. What test can help differentiate a 4th nerve palsy from skew deviation?
The upright-supine test helps differentiate a skew deviation from trochlear nerve palsy: a vertical deviation that decreases by ≥50% from the upright to supine position suggests a skew deviation.
145. What is the ocular tilt reaction?
A combination of:
1. Skew
2. Ocular torsion (both eyes are tilted toward the hypotropic eye)
3. Head tilt (toward the hypotropic eye).
146. What transmission pathway is disrupted in skew deviation and the ocular tilt reaction?
Skew deviation and the ocular tilt reaction occur when there is a disruption of the otolith-ocular pathway in the vestibular nerves, the brainstem, or the cerebellum.
147. What infectious condition can cause a vertical gaze palsy?
Whipple disease can present as a vertical gaze palsy. This rare disorder is often associated with eye movement abnormalities.
148. What is the cause of Whipple disease?
A gram-positive bacillus, Tropheryma whippelii, which mostly resides in the gut.
149. What are the findings of Whipple disease?
Weight loss, diarrhea, arthritis, lymphadenopathy, and fever that may involve and even be confined to the central nervous system. The neurologic involvement includes slowly progressive memory loss with cognitive impairment, oculomasticatory movements (myorhythmia) which is pathognomonic and supranuclear vertical (more than horizontal) gaze palsy.
150. Where are saccadic eye movements initiated?
Saccadic eye movements are initiated in the frontal lobe and parietal lobe eye fields.
151. Where are smooth pursuit eye movements generated?
Smooth pursuit eye movements are generated in higher cortical centers, especially the parieto–occipital–temporal junction.
152. What is the function of inputs to the visual system from the vestibular nuclear complexes?
Conjugate gaze in both the vertical and horizontal planes is stabilized through inputs from the vestibular nuclei.
153. What is Ocular Neuromyotonia?
It is tonic spasms of the extraocular muscles innervated by the third or sixth cranial nerve that occurs during sustained eccentric gaze.
154. What are the symptoms of Ocular Neuromyotonia?
Affected patients complain of episodic diplopia lasting seconds or minutes and occurring after they look in a specific direction for a few seconds. Some patients feel that the eye is pulled in the orbit.
155. What is the usual cause of Ocular Neuromyotonia?
This rare disorder classically develops months or years after radiation involving the ocular motor nerves usually for a pituitary tumor or skull base tumor. Carbamazepine is sometimes helpful.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
Skew Deviation and the Ocular Tilt Reaction

Skew deviation (▶Fig. 13.131) consists of the following:
● Vertical misalignment of the eyes commonly results from acute brainstem dysfunction.
● Patients complain of vertical diplopia, sometimes with a torsional component.
● There are usually other neurologic symptoms.
● The hypertropia of a skew deviation may be comitant (deviation is the same in all positions of gaze) or noncomitant (deviation varies with gaze position). When a skew deviation is noncomitant, it may be difficult to distinguish from a third nerve palsy or fourth nerve palsy.
Ocular tilt reaction (OTR) (▶Fig. 13.132) is a combination of the following:
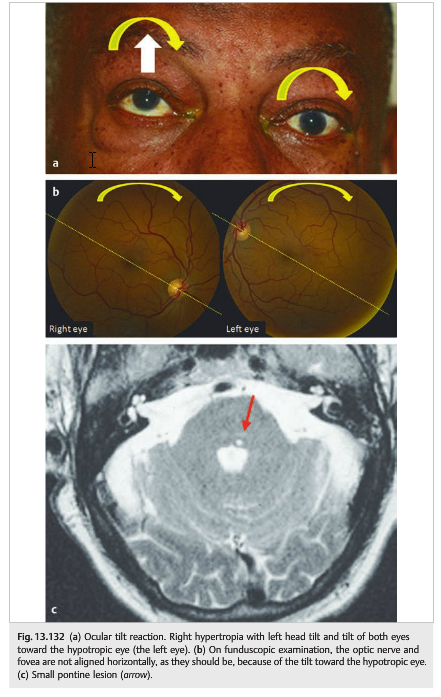
● Skew deviation
● Ocular torsion (both eyes are tilted toward the hypotropic eye) (It is easy to see the ocular torsion on funduscopic examination: the imaginary line drawn between the optic nerve and the fovea appears tilted.)
● Head tilt (toward the hypotropic eye)
● Common with lesions of the pontomedullary junction or the paramedian thalamic–mesencephalic region
● Results from dysfunction of the utricular pathways that begin in the labyrinths and terminate in the rostral brainstem at the INC
● The OTR will be
○ ipsiversive with peripheral and pontomedullary lesions
○ contraversive with pontomesencephalic lesions
Skew deviation and the ocular tilt reaction occur when there is disruption of the otolith-ocular pathway in the vestibular nerves, the brainstem, or the cerebellum.
Classic causes of skew deviation and ocular tilt reaction include the following:
● Acute peripheral vestibulopathy
○ Lesion of the vestibular organ or its nerve
○ Tullio phenomenon: sound-induced vestibular symptoms caused by a perilymph
○ Fistula or abnormalities of the ossicular chain in the ear
● Lesion in the vestibular nuclei (e.g., part of the lateral medullary syndrome)
● Lesion in the cerebellum
● Lesion in the MLF
● Lesion in the midbrain and INC
● Raised intracranial pressure
Control of the Saccade System
Saccadic eye movements (fast conjugate eye movements to a fixed target) are initiated in the frontal and parietal lobes (frontal and parietal eye fields).
● The horizontal saccadic pathway is a crossed pathway. Pathways from the frontal and parietal eye fields descend via the superior colliculus into the brainstem and cross at the level of the midbrain-pontine junction to synapse on the contralateral PPRF.
● The PPRF projects to the ipsilateral sixth nerve nucleus. From the sixth nerve nucleus, axons of abducens motor neurons travel to the ipsilateral lateral rectus muscle, whereas axons of sixth nerve interneurons cross over and ascend in the contralateral MLF to the medial rectus subnucleus of the third nerve.
● This internuclear connection between the sixth nerve nucleus and the contralateral third nerve nucleus via the MLF is responsible for conjugate horizontal gaze.
● Each frontal eye field, therefore, generates a conjugate movement of the eyes toward the contralateral side of the body.
● Brainstem pathways for vertical saccades involve the riMLF, the posterior commissure (PC) and nucleus of the PC, and the INC.
Slow Saccades
Differential diagnosis of slow saccades includes the following:
● Lesions in the pons and the cerebellum
○ Spinocerebellar ataxias
○ Lesions of the PPRF
○ Internuclear ophthalmoplegia
○ Paraneoplastic syndrome
● Lesions in the midbrain
○ Progressive supranuclear palsy
○ Whipple disease
● Lesions in the basal ganglia
○ Parkinson syndromes
○ Huntington disease
○ Creutzfeldt-Jakob disease
● Miscellaneous
○ Medications (anticonvulsants, benzodiazepines)
○ Wilson disease
○ Lipid storage diseases
Control of the Pursuit System
Smooth pursuit eye movements (conjugate maintenance of fixation of the eyes while following a moving target) are generated in higher cortical centers, especially the parieto-occipital–temporal junction.
Inputs are sent from each parieto–occipital–temporal junction to the superior colliculus (SC), which mediate control of horizontal and vertical pursuit eye movements.
Descending horizontal gaze pursuit fibers synapse on the sixth nerve nucleus directly without synapsing in the PPRF.
Unlike the saccadic system, in which each hemisphere (frontal eye fields and other centers) produces conjugate horizontal eye movements toward the contralateral direction because of crossing of the saccadic pathways in the brainstem, the pursuit system is designed such that each hemisphere controls conjugate pursuit eye movements to the ipsilateral visual space.
Vestibulo-ocular System
Conjugate gaze in both the vertical and horizontal planes is stabilized through inputs from the vestibular nuclei.
● From each vestibular nuclear complex, axons subserving horizontal gaze-holding sends an excitatory connection to the contralateral sixth nerve nucleus and an inhibitory projection to the ipsilateral abducens nucleus; motor neurons from the sixth nerve nucleus innervate the lateral rectus, whereas interneurons cross over to ascend in the MLF to the third nerve nucleus. Stimulatory input from each vestibular nucleus, therefore, produces conjugate horizontal gaze toward the contralateral side of the body.
● Inputs from the vestibular nuclei also influence vertical gaze-holding through inputs (some via the MLFs) to the contralateral fourth nerve nucleus, third nerve nucleus, INC, and riMLF. The maintenance of ocular alignment in the vertical plane is controlled by the existence of balanced inputs from the vestibular nuclei to the fourth nerve nucleus (which innervates the contralateral superior oblique muscle), the superior rectus subnucleus (innervates the contralateral superior rectus), and the inferior oblique and inferior rectus subnuclei (innervate the ipsilateral inferior oblique and inferior rectus). An imbalance between these inputs to the various subnuclei results in skew deviation.
13.5.6 Other Eye Movement Abnormalities
Locked-in Syndrome
Large bilateral lesions (essentially transecting the pons) may cause a neurologic state characterized by the combination of the following:
● Quadriplegia
● Absence of horizontal eye movements
● Mutism
● Preservation of vertical eye movements
● Normal blinking
● Normal consciousness
These patients are able to communicate only by using blinking and vertical eye movements.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.