Questions:
104. What diagnoses should be considered in all cases of new-onset constant or transient ptosis and/or diplopia?
105. What syndromes have ataxia, areflexia, and ophthalmoplegia?
106. What is the Miller Fisher syndrome?
107. What is the Guillain-Barré syndrome?
108. What is the difference between the Miller Fisher and the Guillain-Barré syndromes?
109. When should the Wernicke encephalopathy be considered?
110. What is Wernicke encephalopathy?
111. What does botulism do to the pupils and what are its other symptoms?
112. What is the infectious agent of botulism?
113. What is the mechanism of botulism toxin?
114. What is the treatment for botulism?
____________________________________________________
Questions with answers:
104. What diagnoses should be considered in all cases of new-onset constant or transient ptosis and/or diplopia?
Myasthenia, Wernicke syndrome, and if over age 50 cranial arteritis.
105. What syndromes have ataxia, areflexia, and ophthalmoplegia?
The Miller Fisher and the Guillain-Barré syndromes are demyelinating polyradiculopathies that can be associated with multiple cranial nerve palsies and bilateral ophthalmoplegia.
106. What is the Miller Fisher syndrome?
It presents with a classic triad of:
1. ataxia
2. areflexia
3. ophthalmoplegia (bilateral third, fourth, and 6th nerve palsies)
The pupils are often involved.
Bilateral facial weakness is common, but there is no limb weakness.
107. What is the Guillain-Barré syndrome?
It may have the same findings as the Miller Fisher syndrome (ataxia, areflexia, and ophthalmoplegia (bilateral third, fourth, and 6th nerve palsies). The pupils are often involved. Bilateral facial weakness is common. It also includes progressive ascending symmetric limb weakness without sensory loss, which may be complicated by respiratory paralysis.
108. What is the difference between the Miller Fisher and the Guillain-Barré syndromes?
The Guillain-Barré syndrome has progressive ascending limb weakness but the Miller Fisher syndrome does not. They both are demyelinating polyradiculopathies that can be associated with multiple cranial nerve palsies and bilateral ophthalmoplegia, pupillary dysfunction and bilateral facial weakness.
109. When should the Wernicke encephalopathy be considered?
It should be suspected in any patient presenting with: confusion, ataxia, ophthalmoplegia (any pattern is possible, including 6th nerve palsy, horizontal or vertical gaze palsy, internuclear ophthalmoplegia), and nystagmus. Like myasthenia gravis, Wernicke encephalopathy can mimic any extraocular movement disorder with normal pupils.
110. What is Wernicke encephalopathy?
It is a thiamine deficiency that usually occurs as a result of chronic alcoholism and severe chronic malnutrition. It should be suspected in any patient presenting with: confusion, ataxia, ophthalmoplegia. However, only 10% of patients exhibit all three features, and other symptoms may also be present Treatment with vitamin B1, hydration, and appropriate nutrition. Treatment is urgent to prevent irreversible dementia.
111. What does botulism do to the pupils and what are its other symptoms?
There is bilateral mydriasis associated with bilateral ophthalmoplegia, ptosis and systemic signs (nausea, vomiting, dysphagia, proximal extremity weakness).
112. What is the infectious agent of botulism?
Clostridium botulinum (from contaminated canned food or contaminated wounds).
113. What is the mechanism of botulism toxin?
It interferes with the release of acetylcholine vesicles in the synapse and blocks neuromuscular transmission.
114. What is the treatment for botulism?
This life-threatening disorder requires immediate life-support measures and treatment with specific antitoxins.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
Miller Fisher Syndrome and Guillain-Barré Syndrome
Demyelinating polyradiculopathies can be associated with multiple cranial nerve palsies and bilateral ophthalmoplegia.
Miller Fisher syndrome presents with a classic triad:
● Ataxia
● Areflexia
● Ophthalmoplegia (bilateral third, fourth, and sixth nerve palsies; the pupils are often involved)
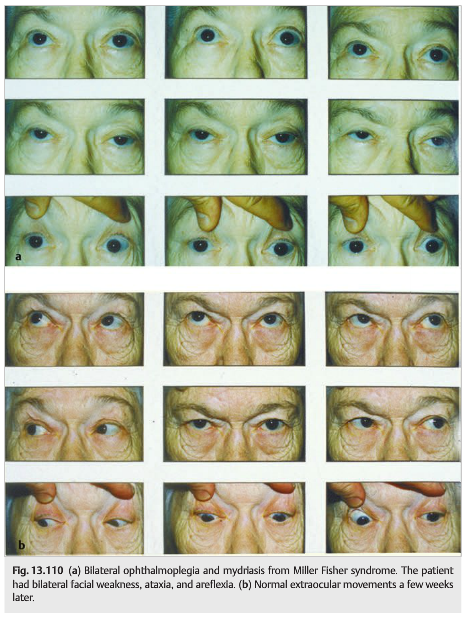
Bilateral facial weakness is common, but there is no limb weakness. The diagnosis is suspected clinically and is confirmed by CSF analysis (elevated protein and few or no cells) and by electromyography. Serum antibodies for Campylobacter jejuni or anti-GQ1b gangliosides may be positive. Prognosis is usually good with supportive measures; treatment with intravenous immunoglobulins or plasmapheresis is usually performed ▶Fig. 13.110).
Guillain-Barré syndrome may have the same clinical presentation as Miller Fisher syndrome but also includes progressive ascending symmetric limb weakness (no sensory loss), which may be complicated by respiratory paralysis.
Wernicke Encephalopathy
Thiamine deficiency usually occurs as a result of chronic alcoholism and severe chronic malnutrition, especially after bariatric surgery. It should be suspected in any patient presenting with the following:
● Confusion
● Ataxia
● Ophthalmoplegia (any pattern is possible, including sixth nerve palsy, horizontal or vertical gaze palsy, internuclear ophthalmoplegia)
● Nystagmus (common)
Brain MRI often shows symmetric increased T2 signal intensity in the mammillary bodies, the medial thalami, the tectal plate, and the periaqueductal area. Treatment With vitamin B1, hydration, and appropriate nutrition is urgent to prevent irreversible dementia.
Pearls
Thiamine deficiency can mimic any extraocular movement disorder; nystagmus is commonly associated.
Botulism
Clostridium botulinum poisoning (from contaminated canned food or contaminated wounds) causes systemic signs (nausea, vomiting, dysphagia, proximal extremity weakness) associated with bilateral diffuse ophthalmoplegia, ptosis, and bilateral mydriasis.
Botulinum toxins interfere with the release of acetylcholine vesicles in the synapse and block neuromuscular transmission.
This life-threatening disorder requires immediate life-support measures and treatment with specific antitoxins.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.