Questions:
92. What signs when associated with lesions causing unilateral or bilateral ophthalmoplegia may help localize the lesion?
93. What are the findings of the orbital apex syndrome?
94. Do brainstem lesions often produce multiple cranial nerve palsies?
95. What are 4 systemic disorders that affect the cranial nerves?
96. What condition should be considered in patients with unilateral or bilateral ophthalmoplegia and normal pupils presumed to result from multiple cranial neuropathies?
97. What is the likely cause of a painful orbital apex syndrome in a diabetic patient?
98. Do normal orbital imaging studies rule out an orbital apex lesion?
99. Does the orbital apex syndrome involve the second division of the fifth nerve?
100. What are the findings of the cavernous sinus syndrome?
101. If a cavernous sinus syndrome includes venous hypertension (carotid-cavernous fistula or cavernous sinus thrombosis), what additional findings may be present?
102. Which cranial nerves are enclosed in the lateral wall of the cavernous sinus?
103. Why do cavernous carotid artery aneurysms often present with an isolated sixth nerve palsy?
____________________________________________________
Questions with answers:
92. What signs when associated with lesions causing unilateral or bilateral ophthalmoplegia may help localize the lesion?
Associated signs (such as Horner syndrome, optic neuropathy, chiasmal visual field defect, pain, skin lesions, and other neurologic findings) help localize the lesion.
93. What are the findings of the orbital apex syndrome?
Orbital apex syndrome: third, fourth, sixth, and fifth (first branch) nerve palsies with optic neuropathy, sometimes with Horner syndrome. Causes include mostly neoplasms and fungal infections (aspergillosis and mucormycosis).
94. Do brainstem lesions often produce multiple cranial nerve palsies?
Brainstem lesions rarely produce multiple cranial nerve palsies (almost always associated with other neurologic symptoms and signs).
95. What are 4 systemic disorders that affect the cranial nerves?
Systemic disorders affecting the cranial nerves:
1. Miller Fisher syndrome
2. Guillain-Barré syndrome
3. Botulism
4. Wernicke encephalopathy
5. Other peripheral neuropathies
96. What condition should be considered in patients with unilateral or bilateral ophthalmoplegia and normal pupils presumed to result from multiple cranial neuropathies?
Always consider ocular myasthenia in patients with unilateral or bilateral ophthalmoplegia and normal pupils presumed to result from “multiple cranial neuropathies.”
97. What is the likely cause of a painful orbital apex syndrome in a diabetic patient?
A painful orbital apex syndrome in a diabetic patient should be presumed caused by a local infection by mucormycosis until proven otherwise.
98. Do normal orbital imaging studies rule out an orbital apex lesion?
Normal orbital imaging studies do not rule out an orbital apex lesion.
99. Does the orbital apex syndrome involve the second division of the trigeminal nerve?
No, the orbital apex syndrome involves sensory loss in the first division of the trigeminal nerve, not the second division.
The orbital apex syndrome consists of ophthalmoplegia (multiple cranial nerve palsies), Horner syndrome, pain and sensory loss in the first division of the trigeminal nerve, and visual loss (optic neuropathy).
100. What are the findings of the cavernous sinus syndrome?
Cavernous sinus syndrome involves combinations of the following: ophthalmoplegia (multiple ocular motor cranial nerve palsies), Horner syndrome, pain, and sensory loss in the first division of the trigeminal nerve and sometimes the second division.
101. If a cavernous sinus syndrome includes venous hypertension (carotid-cavernous fistula or cavernous sinus thrombosis), what additional findings may be present?
There may be proptosis and periorbital edema from orbital venous congestion.
102. Which cranial nerves are enclosed in the lateral wall of the cavernous sinus?
The third, fourth, and fifth nerves (V1 and V2) are enclosed in the lateral wall of the cavernous sinus (made of dura).
103. Why do cavernous carotid artery aneurysms often present with an isolated sixth nerve palsy?
The sixth nerve is free within the cavernous sinus and in close relation with the internal carotid artery and not protected by the dura.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
13.5.4 The Lesion Involves Multiple Cranial Nerves
Lesions involving more than one cranial nerve often produce unilateral or bilateral ophthalmoplegia. Associated signs (such as Horner syndrome, optic neuropathy, chiasmal visual field defect, pain, skin lesions, and other neurologic findings) help localize the lesion.
Classic locations and causes of unilateral or bilateral ophthalmoplegia related to multiple cranial nerve palsies include the following:
● Orbital apex syndrome: third, fourth, sixth, and fifth (first branch) nerve palsies with optic neuropathy, sometimes with Horner syndrome. Causes include mostly neoplasms and fungal infections (aspergillosis and mucormycosis).
● Cavernous sinus lesion: third, fourth, sixth, and often fifth (first branch and sometimes second branch) nerve palsies, sometimes with Horner syndrome. Causes include numerous neoplasms, inflammations, and infections. Aneurysms and carotid-cavernous fistulas are also common.
● Pituitary mass: with expansion into, or compression of, cavernous sinuses (chiasm or optic nerve compression often associated)
● Meningeal process: such as infectious, inflammatory, or neoplastic meningitis
● Skull base lesions: such as infiltrating neoplasms
● Perineural spread: from skin cancers
● Zoster: involving the trigeminal territory
● Brainstem lesions: can rarely produce multiple cranial nerve palsies (almost always associated with other neurologic symptoms and signs).
● Systemic disorders affecting the cranial nerves:
○ Miller Fisher syndrome
○ Guillain-Barré syndrome
○ Botulism
○ Wernicke encephalopathy
○ Other peripheral neuropathies (e.g., chronic inflammatory demyelinating peripheral neuropathy)
Pearls
Always consider ocular myasthenia in patients with unilateral or bilateral ophthalmoplegia and normal pupils presumed to result from “multiple cranial neuropathies.”
Orbital Apex Syndrome
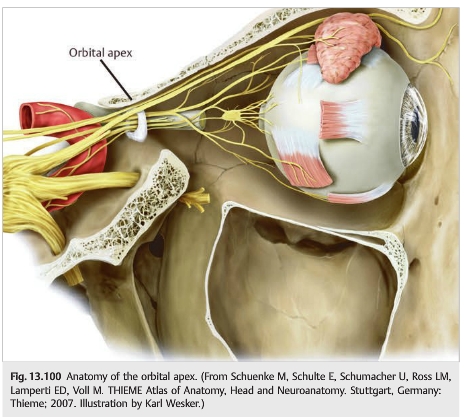
Orbital apex syndrome consists of combinations of the following (▶Fig. 13.100):
● Ophthalmoplegia (multiple cranial nerve palsies)
● Horner syndrome
● Pain and V1 sensory loss (trigeminal nerve)
● Visual loss (optic neuropathy)
Classic causes include the following:
● Neoplasms (metastases, lymphoma)
● Infections (aspergillus, mucormycosis)
Orbital apex lesions are usually very small and are difficult to see on imaging.
The adjacent sinuses are often abnormal, making it even more difficult to see a subtle enhancement on orbital CT or MRI. The appropriate imaging is either a CT scan of the orbits, the cavernous sinus, and the facial sinuses with contrast, or, preferably, a brain MRI scan with dedicated orbital views, fat suppression, and contrast.
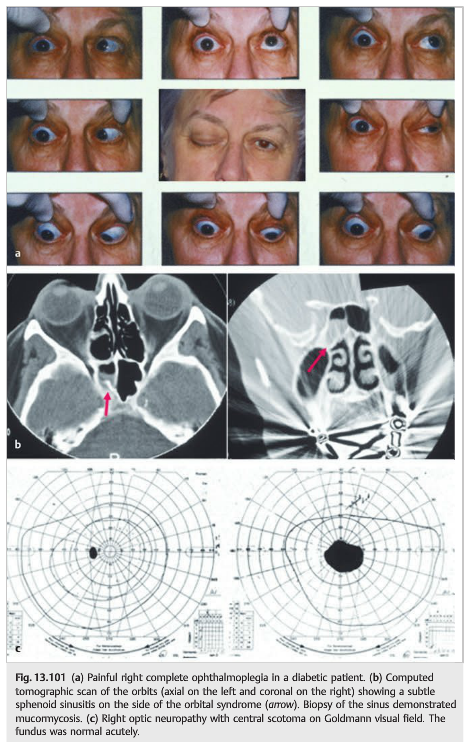
A biopsy (often through the nose and the adjacent sinuses) is often necessary to ensure a proper diagnosis. Diabetic patients have a higher risk of fungal infections, which often originate in or near the facial sinuses. These patients are particularly at risk for a rare, but devastating, infection by mucormycosis.
The sphenoid and the ethmoid sinuses are in very close relation to the orbital apex. Identification of a “sinusitis” on the side of an orbital apex syndrome is highly suspicious for fungal infection. Biopsy for pathology and specific cultures is mandatory (▶Fig. 13.101).
Pearls
● A painful orbital apex syndrome in a diabetic patient should be presumed caused by a local infection by mucormycosis until proven otherwise.
● Normal imaging does not rule out an orbital apex lesion.
Cavernous Sinus Syndrome
Cavernous sinus syndrome involves combinations of the following:
● Ophthalmoplegia (multiple ocular motor cranial nerve palsies)
● Horner syndrome
● Pain and V1 (sometimes also V2) sensory loss
If there is venous hypertension (carotid-cavernous fistula or cavernous sinus thrombosis), there may be proptosis and periorbital edema from orbital venous congestion.
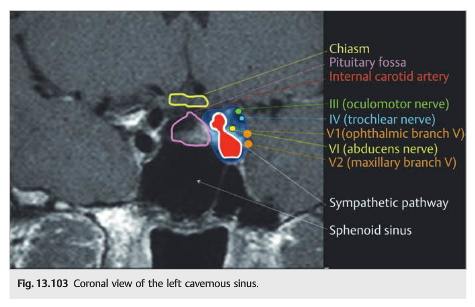
Anatomy of the Cavernous Sinus
The cavernous sinuses are triangular interconnecting structures that flank the lateral sides of the sella turcica (where the pituitary gland resides: (▶Fig. 13.102).

Each cavernous sinus contains a plexus of veins draining the orbits and some of the intracranial veins. The carotid artery (surrounded by sympathetic fibers) passes through the cavernous sinus. All ocular motor cranial nerves traverse the cavernous sinus before entering the orbit.
Tumors and vascular lesions of the cavernous sinus are common and typically present with ophthalmoplegia from ipsilateral third, fourth, and sixth nerve paresis.
Pain is common because the first division of the fifth nerve (trigeminal nerve) is also commonly affected (▶Fig. 13.103).
Pearls
● The third, fourth, and fifth nerves (V1 and V2) are enclosed in the lateral wall of the cavernous sinus (made of dura).
● The sixth nerve is free within the cavernous sinus and in close relation with the internal carotid artery. This is why cavernous carotid artery aneurysms often present with an isolated sixth nerve palsy.
● The internal carotid artery is covered by sympathetic fibers in the cavernous sinus. A lesion of the carotid artery compressing the sixth nerve usually also gives rise to an ipsilateral Horner syndrome.
Causes of Cavernous Sinus Syndrome
Common causes of cavernous sinus syndrome include the following:
● Neoplasms:
○ Meningioma
○ Pituitary tumor
○ Lymphoma
○ Metastasis
○ Other neoplasms
● Carotid-cavernous aneurysm
● Carotid-cavernous fistula
● Abscess
● Fungal infection
● Inflammation:
○ Sarcoidosis
○ Wegener granulomatosis
○ Nonspecific (so-called Tolosa-Hunt syndrome)
Cavernous sinus meningiomas represent the most common cause of cavernous sinus lesions. There is little pain unless the trigeminal nerve is involved ▶Fig. 13.104).

Lesions of the cavernous sinus cannot be easily biopsied, and the diagnosis is sometimes difficult to confirm.
The term Tolosa–Hunt syndrome is sometimes used to describe painful ophthalmoplegia with enhancement of the cavernous sinus. The pain and ophthalmoplegia are exquisitely responsive to treatment with steroids, and the presumed mechanism of the lesion is nonspecific inflammation. However, patients with malignant neoplasms (such as metastasis or lymphoma) or infection (such as aspergillosis or mucormycosis) may have a similar clinical and radiologic presentation and similar response to steroids, making the diagnosis of Tolosa–Hunt syndrome often misleading, erroneously reassuring, and frequently wrong (▶Fig. 13.105).

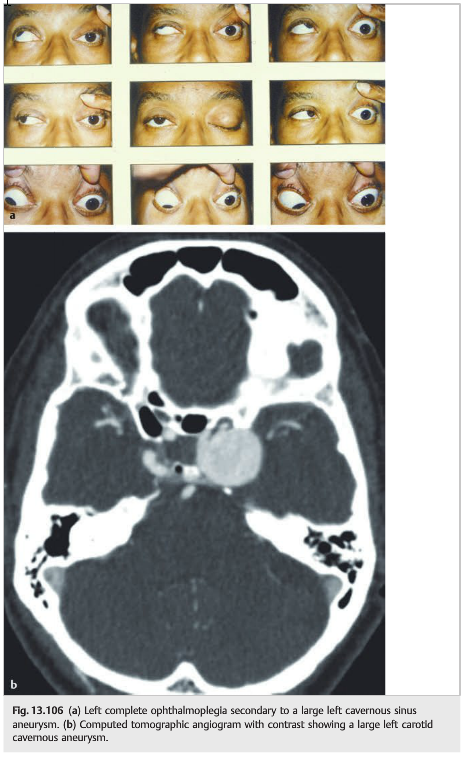
Cavernous sinus aneurysms are relatively common and classically present with isolated unilateral sixth nerve palsy associated with an ipsilateral Horner syndrome. When the aneurysm enlarges, complete ophthalmoplegia may develop.
These aneurysms are usually not life threatening. Their rupture rate is low, and when they do rupture, they do not result in subarachnoid hemorrhage (they rupture inside the cavernous sinus, which is an enclosed space), but rather the rupture causes a direct carotid-cavernous fistula (▶Fig. 13.106).
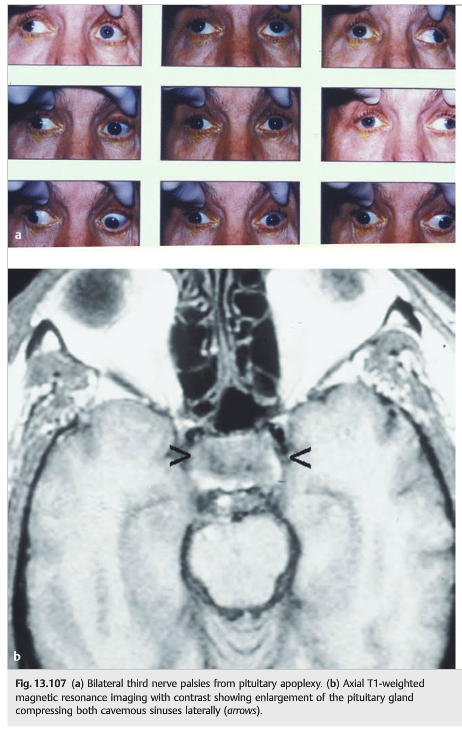
Pituitary Tumors and Pituitary Apoplexy
Pituitary masses compressing or invading the cavernous sinus are a common cause of unilateral or bilateral ophthalmoplegia (the pituitary gland is located between the two cavernous sinuses).Pituitary apoplexy (acute pituitary hemorrhage or infarction, usually in a preexisting, although often unrecognized, pituitary tumor) classically results in sudden unilateral or bilateral ophthalmoplegia, headache, and often visual loss (from compression of the optic nerves and chiasm) (▶Fig. 13.107).
Trigeminal Zoster
Trigeminal zoster is a rare cause of ophthalmoplegia (▶Fig. 13.108).

Severe varicella zoster virus infection involving the V1 territory can rarely produce a single or multiple cranial nerve palsy on the same side. The presumed mechanism is extension of the inflammatory reaction into the cavernous sinus. However, orbital myositis is sometimes seen on imaging. These patients often require prolonged treatment with antiviral agents and corticosteroids.
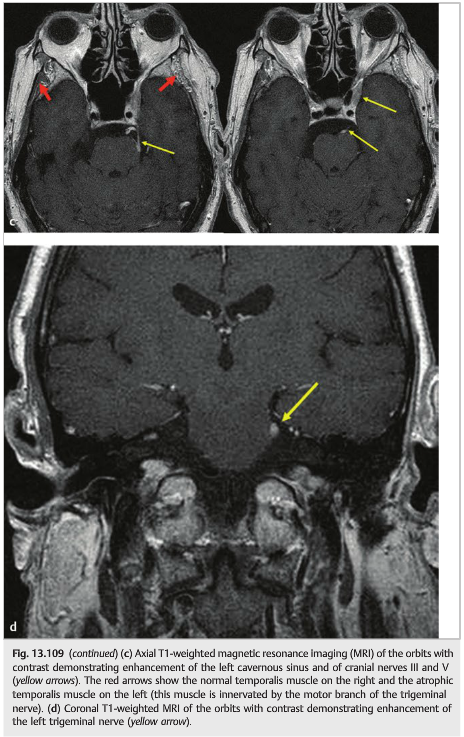
Cutaneous Squamous Cell Carcinomas or Basal Cell Carcinomas
Cutaneous squamous cell carcinomas or basal cell carcinomas located on the face can spread to the Perineural space along the cranial nerves. They produce progressive painful ophthalmoplegia, which is often misdiagnosed for months or even years (▶Fig. 13.109).

Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.