Questions:
125. What is congenital ocular motor apraxia?
126. What is convergence spasm?
127. What is the cause of convergence spasm?
128. What test will usually differentiate convergence spasm from a bilateral 6th nerve palsy?
129. What is convergence insufficiency?
130. How is convergence insufficiency treated?
131. What are causes of convergence insufficiency?
132. What is divergence insufficiency?
133. What causes divergence insufficiency?
134. What lesion location is likely in the presence of horizontal conjugate deviation of the eyes to one side?
_________________________________________________________________
Questions with answers:
125. What is congenital ocular motor apraxia?
It is seen in young children who have a defect or absence of voluntary horizontal saccades to visual stimuli. They use head thrusts to shift fixation.
126. What is convergence spasm?
It is spasm of the near triad:
1. Intermittent convergence
2. with accommodation
3. pupillary constriction
When the patient is asked to look to each side, the eyes do not move.
127. What is the cause of convergence spasm?
Classically convergence spasm is nonorganic. It may be seen with excessive accommodation from uncorrected refractive error and very rarely with lesions at the diencephalic–mesencephalic junction.
128. What test will usually differentiate convergence spasm from a bilateral 6th nerve palsy?
Ductions should be tested with the fellow eye covered. With one eye covered, the patient is able to move the open eye laterally and the pupil will dilate.
129. What is convergence insufficiency?
It is very a common condition where there is a comitant exotropia greater at near than at distance by at least 10 prism diopters. It produces symptoms of asthenopia, fatigue with reading, diplopia at near, and intermittent blurred vision when reading. It is usually benign.
130. How is convergence insufficiency treated?
A common a daily, home rehabilitation technique is to have the patient do “push-up exercises” (looking at an object intermittently moved in and out from the bridge of the nose) to decrease the near point of convergence. Prism in reading glasses or strabismus surgery may be required.
131. What are causes of convergence insufficiency?
1. It is idiopathic most often in children or young adults
2. Head trauma
3. Parkinson disease
4. Progressive supranuclear palsy.
132. What is divergence insufficiency?
Divergence insufficiency is a comitant esotropia that is present at distance but not at near, with full ductions and versions.
133. What causes divergence insufficiency?
It is most often related to raised intracranial pressure or Chiari malformation. It can also be seen with head trauma, intracranial hypotension, cerebellar lesions, and a midbrain mass.
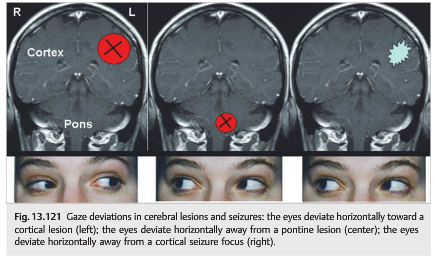
134. What lesion locations are likely in the presence of horizontal conjugate deviation of the eyes to one side?
Horizontal conjugate deviation of the eyes may be found with acute lesions of either hemisphere or the brainstem. The eyes deviate horizontally toward a cortical lesion, the eyes deviate horizontally away from a cortical seizure focus, and the eyes deviate horizontally away from a pontine lesion.
_________________________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
Congenital Ocular Motor Apraxia
● It affects young children.
● Defective or absence of voluntary horizontal saccades to visual stimuli: they cannot move their eyes horizontally to look at a target. Instead they turn their head briskly (head thrust) to shift fixation.
● Smooth pursuit and vertical eye movements are usually preserved.
● Eye movements are usually bilateral and symmetric in the horizontal plane.
● It is often idiopathic, but it has also been associated with several cerebral malformations and genetic disorders.
Acquired Ocular Motor Apraxia
● Occurs in older children
● Associated with mostly metabolic disorders (Gaucher disease, ataxia-telangiectasia, spinocerebellar ataxias, Niemann–Pick disease)
Convergence Spasm
Also called spasm of the near triad (▶Fig. 13.119)

● Intermittent convergence
● Always with accommodation and pupillary constriction
Classic causes of convergence spasm include the following:
● Most often nonorganic
● Excessive accommodation from uncorrected refractive error
● Lesions at the diencephalic–mesencephalic junction (very rare)
Convergence Insufficiency
Convergence insufficiency is a very common condition, characterized by the following:
● Exotropia greater at near than at distance (at least 10 prism diopters difference)
● Causes symptoms of “asthenopia” (fatigue with reading, diplopia at near, intermittent blurred vision when reading)
● Usually benign; may improve with orthoptic exercises
● Sometimes requires prisms in reading glasses or strabismus surgery
Classic causes of convergence insufficiency include the following:
● Idiopathic most often (in children or young adults)
● Head trauma
● Parkinson disease
● Progressive supranuclear palsy
The ability to converge can be measured (▶Fig. 13.120). A near card is brought toward the patient’s nose until the patient sees double. The distance at which diplopia occurs is noted (near point of convergence).
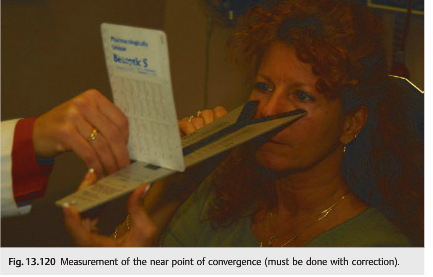
A similar technique is used for rehabilitation: the patient is instructed to do “push-up exercises” (looking at an object intermittently moved in and out from the bridge of the nose) daily at home to decrease the near point of convergence.
Divergence Insufficiency
Divergence insufficiency is characterized as follows:
● Comitant esotropia is present at distance but not at near.
● Ductions and versions are full.
● It is most often related to raised intracranial pressure or Chiari malformation.
Classic causes of divergence insufficiency include the following:
● Raised intracranial pressure
● Chiari malformation
● Head trauma
● Intracranial hypotension (low CSF pressure syndrome)
● Cerebellar lesions
● Midbrain mass
Abnormal Horizontal Conjugate Deviations
Gaze deviations are relatively common in large cerebral and pontine lesions (▶Fig. 13.121).
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.