Questions:
13. How is Bell’s phenomenon checked in normal patients?
14. What is the localization of the lesion in a patient when Bell’s phenomenon is preserved despite an upgaze paresis?
15. What is the localizing value of abnormal eye movements that are overcome by oculocephalic maneuvers?
16. What symptom is usually noted by a patient with convergence insufficiency?
17. A patient presents with a history of the onset of diplopia 3 weeks ago. What should be the first characteristic of the diplopia determined?
18. Your exam confirms that a patient has binocular diplopia, but on exam the extraocular movements appear full. What must be present?
19. Your exam confirms that a patient has patient binocular diplopia, but on exam the extraocular movements appear full. What tests will be helpful in demonstrating the misalignment?
20. What will the cross-cover test detect that the cover-uncover test will not detect?
21. When is a phoria pathologic and not physiologic?
22. Is the 3-step-test useful in horizontal or vertical binocular diplopia?
23. What reflex is involved in the third step of the 3-step-test?
24. With the red Maddox rod placed between a light source and the eye, what does the eye see?
25. Why would one perform the double Maddox Rod test?
26. When are the Hirschberg and Krimsky tests useful?
27. How is the Hirschberg test performed?
28. How is the Krimsky test performed?
____________________________________________________
Questions with answers:
13. How is Bell’s phenomenon checked in normal patients?
In normal patients, it can be checked by having the patient try to close the eyes while the examiner holds the lids open. If the eyes move upwards the phenomenon is intact.
14. What is the localization of the lesion in a patient when Bell’s phenomenon is preserved despite an upgaze paresis?
This indicates the presence of a supranuclear defect with intact nuclear and infranuclear function (e.g. Parinaud dorsal midbrain syndrome). It is not preserved in a complete 3rd nerve palsy or myopathy.
15. What is the localizing value of abnormal eye movements that are overcome by oculocephalic maneuvers? The defect is most likely a supranuclear lesion but it can also be nonorganic.
16. What symptom is usually noted by a patient with convergence insufficiency?
Binocular horizontal diplopia when reading. These patients develop an exotropia at near.
17. A patient presents with a history of the onset of diplopia 3 weeks ago. What should be the first characteristic of the diplopia determined?
Determine if the diplopia is binocular or monocular.
18. Your exam confirms that a patient has patient binocular diplopia, but on exam the extraocular movements appear full. What must be present? Ocular misalignment must be present. This usually means that you were not able to visualize a small extraocular motor deficit.
19. Your exam confirms that a patient has patient binocular diplopia, but on exam the extraocular movements appear full. What tests will be helpful in demonstrating the misalignment?
Cover-uncover, Cross-cover and the Maddox rod tests
20. What will the cross-cover test detect that the cover-uncover test will not detect?
The cross-cover test is used to determine if there is latent misalignment (phoria) that is not revealed by the cover-uncover test.
21. When is a phoria pathologic and not physiologic?
Phorias, particularly exophorias, are so common in normal individuals that they may be considered physiological unless the misalignment is incomitant.
22. Is the 3-step-test useful in horizontal or vertical binocular diplopia?
Vertical
23. What reflex is involved in the third step of the 3-step-test?
The vestibulo-ocular reflex (VOR). When the head rotates about any axis (horizontal, vertical, or torsional) distant visual images are stabilized by rotating the eyes about the same axis, but in the opposite direction.
24. With the red Maddox rod placed between a light source and the eye, what does the eye see?
The eye sees an image of a straight red line oriented at 90 degrees to the axis of the cylinders of the Maddox rod.
25. Why would one perform a double Maddox Rod test?
To quantify cyclotorsion.
26. When are the Hirschberg and Krimsky tests useful?
In noncooperative patients or in children.
27. How is the Hirschberg test performed?
With the patient fixating a light at 33 cm., the number of millimeters the corneal light reflex is from the center of the cornea is measured/estimated in the deviating eye (1 mm decentration = 7 degrees = 14 prism-diopters).
28. How is the Krimsky test performed?
With the patient fixating a light at 33 cm., the deviation is measured using prisms of increasing power are to move the deviation of the light reflex until it is centered in each pupil, giving the number of prism diopters of the deviation.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
Bell Phenomenon
With eye closure, there is a normal upward rotation of the eye. This is called the Bell phenomenon. It keeps the cornea from being exposed during sleep.
This normal reflex is easily visible in patients with peripheral facial nerve paralysis who attempt to shut their eyes (▶Fig. 13.14).

In normal patients, it can be checked by having the patient try to close the eyes while the examiner holds the lids open. In a patient with limited up gaze, a normal Bell phenomenon indicates a supranuclear defect with intact nuclear and infranuclear function (e.g., the Bell reflex is preserved despite up gaze paresis in Parinaud (dorsal midbrain) syndrome but is absent in a complete third nerve palsy or myopathy).
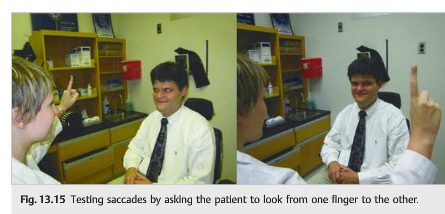
Saccades
Saccades, or fast eye movements, are tested by having the patient refixate between two targets. This can be easily performed by having the patient look at the examiner’s nose and then at an eccentrically placed finger: “look at my nose, look at my finger” (▶Fig. 13.15).
Pursuit
To test the pursuit system, the patient is asked to keep his or her head still and to follow a target (the examiner’s finger) (“follow my finger”).
Oculocephalic Responses
Oculocephalic responses are used to test the vestibulo-ocular reflex and need to be tested in all patients with horizontal or vertical gaze paresis. Normally, the eyes should deviate conjugately in the direction opposite the head turn (▶Fig. 13.16). Oculocephalic responses should not be tested in trauma patients who may have spinal lesions. Abnormal eye movements that are overcome by oculocephalic maneuvers are likely supranuclear (or nonorganic).

Vergences
Vergences are binocular eye movements in which the two eyes move in opposite directions (the eyes need to converge to see a single image at near, and need to diverge to see a single image at distance). Convergence can be evaluated by having the patient look at his or her thumb or other accommodative target as it is brought toward the nose. Both eyes should adduct and there will be pupillary constriction and accommodation of the lens (the “near triad”)(▶Fig. 13.17). Convergence insufficiency is a common cause of binocular horizontal diplopia when the patient is reading. Patients develop an exotropia at near (to be discussed).

13.4.2 Assessing Ocular Misalignment
When a patient complains of binocular diplopia, there must be ocular misalignment. If you conclude that the “extraocular movements are full,” it usually means that you were not able to visualize small extraocular motor deficits. This is when the cover–uncover test, the cross-cover test, the red glass test, or the Maddox rod test becomes very helpful.
The Cover–Uncover Test
This test is based on evoking a fixational eye movement. In nearly all cases of ocular misalignment, one eye fixates the target while the other deviates. If the fixating eye is covered, the deviating eye will move to fixate the target. This test requires good vision and an attentive patient.
Procedure
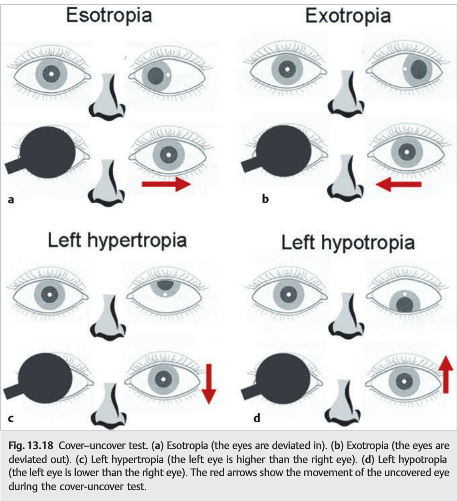
The patient is instructed to fixate on a distant target while the right eye is covered. The left eye is observed to determine if it makes a fixational saccade toward the straight-ahead (primary) position. The direction of movement must be noted. Following removal of the cover from the right eye and after a delay of a few seconds, the left eye is covered and the right eye is watched for a fixational movement (▶Fig. 13.18). This cover-uncover maneuver should be repeated on each eye until the observations are consistent. If a fixational eye movement repeatedly occurs in the same direction, a“manifest misalignment” or a “tropia” can be diagnosed as follows:
● An outward movement denotes a convergent misalignment, or esotropia.
● An inward movement denotes a divergent misalignment, or exotropia.
● A downward movement denotes a hypertropia.
● An upward movement denotes a hypotropia.
The type of misalignment in primary position, right, left, up, and down gaze should be noted (see ▶Fig. 13.18).
The Cross-Cover Test
This test is used to determine if there is latent misalignment not revealed by the cover–uncover test. It is based on eliciting a fixational eye movement, like the cover–uncover test. However, it interferes with binocular vision to bring out any latent misalignments that might be suppressed by a force called binocular fusion. This force is normally exerted to avoid double vision when both eyes are viewing a target.
Procedure
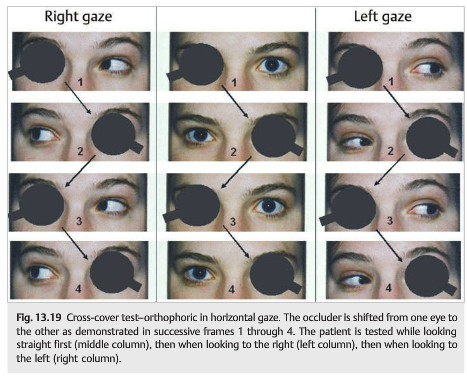
After covering the right eye as before, and after a 1 second pause, the cover is quickly moved across the nasal bridge to cover the left eye. Pausing 1 second, the cover is shifted back to cover the right eye, then the left eye, and so on, alternately covering the two eyes. One observes whether the eye being uncovered is shifting its position, the observations being recorded as with the cover–uncover maneuver. If a consistent fixational eye movement that was not present with the cover–uncover test is elicited, a latent misalignment, or phoria, is identified. Phorias, particularly exophorias, are so common in normal individuals that they may be considered physiological unless the degree of misalignment is incomitant (i.e., varies from one gaze position to another). When the cross-cover test does not elicit any eye movement, the patient is said to be orthophoric (▶Fig. 13.19).
The test is repeated in all directions of gaze to make sure that the patient is orthophoric in right, left, up, and down gazes (▶Fig. 13.20).

In the patient with a complaint of horizontal diplopia, the cross-cover test may show an abduction deficit (▶Fig. 13.21).

In the patient with a complaint of new vertical diplopia, the three-step test is critical in looking for a fourth nerve palsy (▶Fig. 13.22).
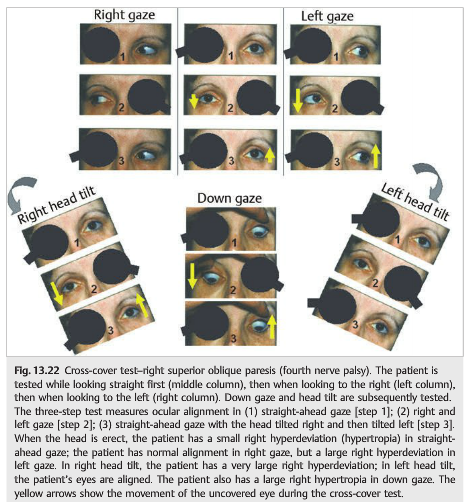
● Step 1: Because there is a right hyperdeviation in straight-ahead gaze, there must be a deficit in the depressor muscles of the right eye (inferior rectus, superior oblique) or the elevator muscles of the left eye (superior rectus, inferior oblique).
● Step 2: If the hyperdeviation is greater on left gaze than on right gaze, a vertical muscle active in left gaze is weak—either the right superior oblique or the left superior rectus.
● Step 3: Tilting the head to either side evokes an otolith-mediated ocular righting response (“ocular tilt reaction”) designed to keep the eyes close to the plane of the horizon. In the right head tilt position, the right eye needs to intort (superior oblique, superior rectus), and the left eye needs to extort (inferior oblique, inferior rectus). If the right eye’s superior oblique is weak, then the only available “intorter” in that position is the intact right superior rectus. Because the primary action of the superior rectus is elevation, the depressor force of the weak superior oblique will be overwhelmed by the elevator force of the intact superior rectus, and the right globe will move upward. As for the left eye, its intact inferior oblique upward pull is neutralized by its intact inferior rectus downward pull, so the globe does not move vertically. Left head tilt evokes an ocular counter-rolling motion that uses four intact muscles, so that neither eye moves vertically.
Quantification of the Ocular Deviation
The ocular misalignment can be quantified by determining the power of the prism necessary to neutralize the ocular deviation (▶Fig. 13.23).

The prism is placed over one eye, with the apex of the prism (point) pointed in the direction in which the eye is deviated: base out for an esotropia, base in for an exotropia, and base down on the right eye for a right hypertropia (▶Fig. 13.24; “the apex of the prism points toward the deviation”).

Each eye is then alternatively covered as the amount of prism (measured in prism-diopters) is slowly increased. When the eyes no longer move on alternate-cover testing, the deviation has been neutralized and the amount of prism required can be read on the prism or the prism bar. This measurement can be done in all cardinal positions and at near, as well as with head tilt.
Pearls
Measurement of the ocular deviation in prism-diopters reliably quantifies the ocular deviation. It is very useful for follow-up and to verify stability prior to considering eye muscle surgery for diplopia.
The same technique of prism quantification can be used during the red glass test or the Maddox rod test. With horizontal and vertical deviations, the same prism techniques can be used, and prisms of different orientations can be combined at the same time.
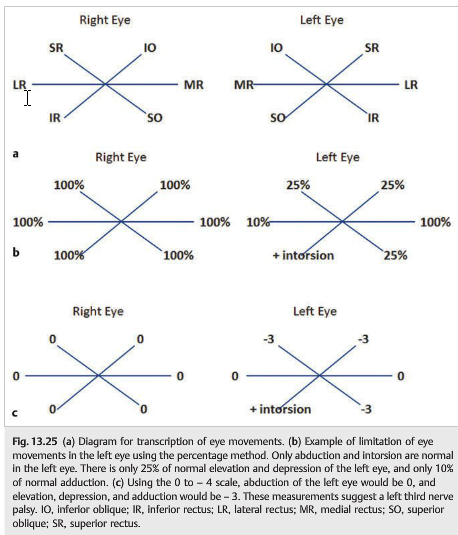
Communicating the Results of the Examination
The eye movements can be described in several ways (▶Fig. 13.25 and ▶Fig. 13.26).

The Red Glass Test
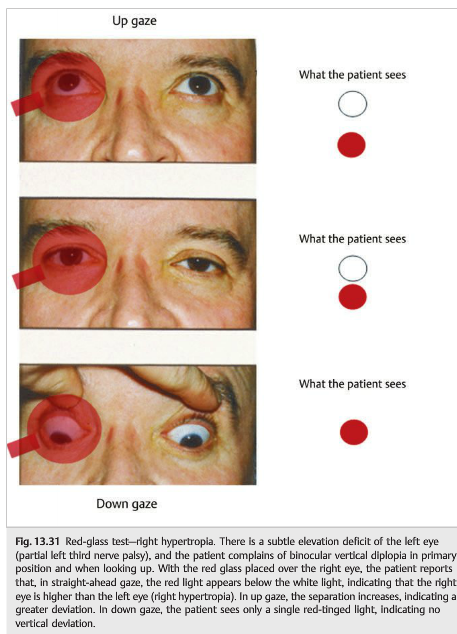
The red glass test relies on the patient’s ability to report the location of two different-colored lights. By convention the red filter is placed in front of the right eye (▶Fig. 13.27).


This maneuver is then repeated for all the relevant positions of gaze (▶Fig. 13.28).
The patient is requested to stare straight ahead at a bright light. If the eyes are aligned, the patient will report one red-tinged light; however, if they are out of alignment, the patient describes one white and one red light. The extent of separation of images horizontally and vertically is determined.
With an esotropia or esophoria, the red image (as seen by the right eye) will appear to the patient as displaced to the right of the white image (▶Fig. 13.29).

With an exotropia or exophoria, the red image (as seen by the right eye) will appear to the patient as displaced to the left. One way to remember this rule of horizontal misalignment is that there is an X in exotropia. This means that the red image viewed by the right eye crosses over to the left of the white light in an exotropia (▶Fig. 13.30).

With a right hypertropia (▶Fig. 13.31), the red image will appear displaced below the white image; with a left hypertropia, the red image will appear displaced above the white image. One way to remember the rule for vertical deviations is that there is an R in sunrise. The red image sits below the white light (the sun) in a right hypertropia.
The red glass test is more sensitive to small amounts of misalignment than the cover test, but it requires an attentive and verbally adept patient. Some patients have difficulty estimating spacing intervals, especially when the eyes are misaligned in two planes; the red glass test using the Maddox rod improves reliability under these circumstances.
The Maddox Rod Test
The Maddox rod itself consists of a stack of transparent red plastic cylinders. When placed between a light source and the eye, it produces an image of a straight red line oriented at 90 degrees to the axis of the cylinders (▶Fig. 13.32).
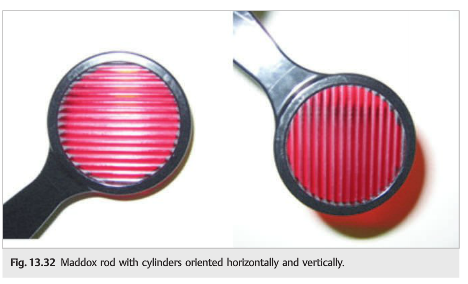
Thus, when the Maddox rod is held before the eye with cylinders oriented vertically,the viewer sees a point light source as a horizontal red line. When the Maddox rod cylinders are oriented horizontally, the red line is seen as vertical. This optical phenomenon allows the examiner to assess misalignment first in the horizontal plane, then in the vertical plane.
13.4.3 Testing for Horizontal and Vertical Deviation
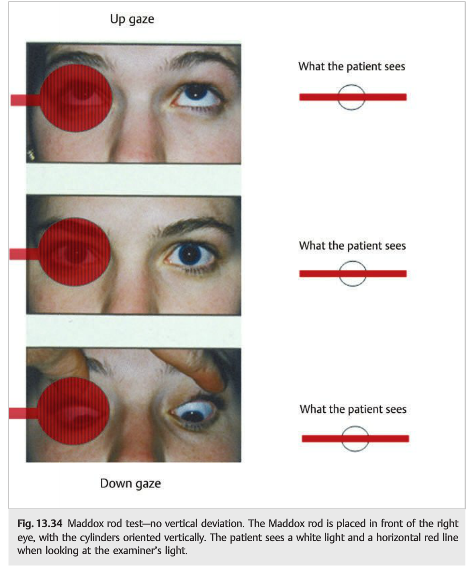
The Maddox rod is used in the same way as the red glass, except that the patient is tested in all relevant gaze positions twice—first with the cylinders oriented horizontally and then with the cylinders oriented vertically (▶Fig. 13.33 and ▶Fig. 13.34).

For horizontal deviations, the Maddox rod is placed in front of the right eye with the cylinders oriented horizontally. When there is no horizontal ocular deviation (orthophoric), the patient sees the light through the red line. When the line is seen to the right of the light (uncrossed diplopia), there is an esotropia (▶Fig. 13.35).

When the line is seen to the left of the light (crossed diplopia), there is an exotropia (▶Fig. 13.36).

For vertical deviations, the Maddox rod is placed in front of the right eye, with the cylinders oriented vertically; the patient looks at the examiner’s light. The patient sees a white light and a horizontal red line. When there is no vertical ocular deviation(orthophoric), the patient sees the light through the red line (see ▶Fig. 13.34).
When the light is seen above the line, there is a right hypertropia (▶Fig. 13.37).

When the light is seen below the line, there is a right hypotropia (or left hypertropia).
Testing for Cyclotorsion
The double Maddox rod test helps demonstrate and quantify cyclotorsion: Maddox rod lenses are placed over each eye in a trial frame (by convention, red in front of right eye and white in front of left eye), with the cylinders oriented vertically (each at the 90 degree mark). As the patient is viewing a hand-held light at distance, two separate horizontal lines will be seen, one with each eye (right eye: red line; left eye: white line). The patient is asked to align the two lines so that they are parallel to each other and the floor by rotating the dials of the trial frame (▶Fig. 13.38 and ▶Fig. 13.39).

13.4.4 Testing Uncooperative Patients or Young Children● Observe spontaneous eye movements and eye position to determine whether the ocular alignment is normal.
● Use the Hirschberg test (corneal reflection test).
● Try the uncover–cover test with a noisy target such as a toy.
The Hirschberg and Krimsky Tests
In uncooperative patients or in children, ocular deviations can be assessed using corneal reflexes. When a fixation light is held 33cm from a patient, the corneal light reflex should be centered in each pupil and should be symmetric. When the light reflex is deviated from the center of the pupil, there is a tropia (▶Fig. 13.40).

Hirschberg test: the deviation of the corneal light reflex from the center of the pupil can be estimated in millimeters (see green arrow in ▶Fig. 13.41):
1mm decentration=7 degrees of ocular deviation=14 prism-diopters

The deviation of the light reflex is measured as follows:
● Edge of pupil: 15 degrees=30 prism-diopters
● Middle iris: 30 degrees=60 prism-diopters
● Edge of iris: 45 degrees=90 prism-diopters
Krimsky test: using the Hirschberg test, prisms of increasing power can be placed in front of the fixating eye until both corneal reflexes are centered. The prism with sufficient power to achieve centration of the light reflex indicates the magnitude of the deviation (▶Fig. 13.42).

● Esotropia: orient the prism base out● Exotropia: orient the prism base in● Hypertropia: orient the prism base up (over the fixating eye); most often patients fixate with the normal eye (the hypertropic eye is deviated upward); hence the need to place the prism base up over the normal fixating eye.● Hypotropia: orient the prism base down (over the fixating eye); most often patients fixate with the normal eye (the hypotropic eye is deviated downward); hence the need to place the prism base down over the normal fixating eye.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.