Questions:
32. What are ocular disorders that keep a large pupil from constricting?
33. How does one test for pharmacologic mydriasis from topical agents?
34. What are two conditions that cause mydriasis via the parasympathetic nervous system?
35. What are the clinical symptoms and signs of Adie tonic pupil?
36. What explains the light-near dissociation classically found in Adie tonic pupil syndrome?
37. What topical drop is used to confirm the presence of Adie pupil syndrome?
38. Is isolated mydriasis likely to be caused by a third nerve paresis?
39. What may happen to the size of the pupil over time in the Adie syndrome?
40. Do all third nerve paresis have pupillary involvement?
41. What may the workup for an isolated third nerve palsy with mydriasis reveal?
____________________________________________________
Questions with answers:
32. What are ocular disorders that keep a large pupil from constricting?
Ocular conditions that keep the large pupil from constricting include posterior synechia, angle-closure glaucoma, previous ocular surgery, ocular trauma, pseudoexfoliation syndrome, and chronic mydriatic use.
33. How does one test for pharmacologic mydriasis from topical agents?
1. Place two drops of dilute pilocarpine (0.1%) in both eyes to make sure this is not an Adie tonic pupil (in which case, the dilated pupil will constrict because of denervation hypersensitivity, whereas the normal or pharmacologic pupil will not change).
2. If there is no response after 45 minutes, place two drops of pilocarpine 1% or 2% in each eye. The normal pupil will constrict. If the dilated pupil constricts only partially or not at all, the diagnosis of pharmacologic mydriasis is confirmed.
34. What are two conditions that cause mydriasis via the parasympathetic nervous system?
Third nerve palsies and Adie tonic pupil syndrome cause mydriasis via the parasympathetic nervous system. Parasympathetic fibers for pupillary constriction travel along the third cranial nerve to the ipsilateral ciliary ganglion within the orbit. Adie tonic pupil syndrome is due to ciliary ganglion dysfunction.
35. What are the clinical symptoms and signs of Adie tonic pupil?
● A large pupil that does not react or reacts poorly to light
● Better constriction when looking at a near target
● Slow tonic redilation of the pupil from near to distance
● Patients often complain of blurry vision at near (accommodation paralysis) and sensitivity to light (from the large pupil).
36. What explains the light-near dissociation classically found in Adie tonic pupil syndrome?
The ratio of fibers that serve accommodation compared with pupil constriction is about 30:1. There is an overwhelming amount of regenerating accommodative fibers that respond to a near stimulus but may aberrantly regenerate to the pupil sphincter muscle; this explains the light-near dissociation classically found in a tonic pupil.
37. What topical drop is used to confirm the presence of Adie pupil syndrome?
0.1% pilocarpine
38. Is isolated mydriasis likely to be caused by a third nerve paresis?
No. Mydriasis from isolated third nerve palsy is essentially always associated with an extraocular movement deficit (responsible for diplopia) and/or ptosis.
39. What may happen to the size of the pupil over time in the Adie syndrome?
Over time, tonic pupils tend to become small (mnemonic =”little old Adies”).
40. Do all third nerve paresis have pupillary involvement?
Not all third nerve palsies have pupil involvement. Pupil involvement is common in nuclear, fascicular, and subarachnoid third nerve palsies. This is because the pupillary fibers are located superficially, they are vulnerable to compressive processes such as aneurysmal mass effect, various tumors such as pituitary apoplexy, and uncal herniation. The evaluation of the patient with a third nerve palsy depends on associated symptoms and signs, the pattern of oculomotor nerve involvement, and the age of the patient.
41. What may the workup for an isolated third nerve palsy with mydriasis reveal?
An isolated third nerve palsy with mydriasis may reveal an intracranial aneurysm or pituitary apoplexy, especially if associated with acute headache.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
Mydriasis (the Large Pupil Is Abnormal)
When the larger pupil does not constrict as well as the small pupil in light, then the large pupil is abnormal (mydriasis). The clinical history and associated symptoms or signs, such as visual loss, diplopia, and ptosis, help in the diagnosis.
Investigations should be obtained only once the mechanism of mydriasis is understood. Indeed, the noncontrast head CT routinely ordered in the emergency room for a patient with mydriasis is useless and falsely reassuring.
Causes
Ocular Disorders
Ocular conditions that keep the large pupil from constricting (e.g., posterior synechia, angle closure glaucoma, previous ocular surgery, ocular trauma, pseudoexfoliation syndrome, and chronic mydriatic use) can produce mydriasis of various sizes; the pupil is not or is poorly reactive to light.
Pupillary dilation following ocular trauma often results from injury to the pupillary sphincter muscle. The pupil may be irregular and is typically large. Its reaction to light and accommodation varies, depending on the extent of the damage. Anisocoria is more evident in bright light as the pupil fails to constrict due to injury to the sphincter muscle. The pupillary abnormality is isolated without ptosis or diplopia.
Pharmacologic Mydriasis
Pharmacologic agents are a common cause of isolated unilateral or bilateral mydriasis. Drugs can produce mydriasis either by stimulation of the sympathetic innervation of the dilator pupillae or by inhibition of the parasympathetic innervation to the sphincter pupillae. Topical agents (e.g., ocular drops or toxins accidentally or purposely placed in the eye) usually cause a unilateral mydriasis, and systemic agents can cause bilateral mydriasis (▶Table 12.5 and ▶Table 12.6).


Pharmacologic mydriasis can also occur when the patient touches a substance with effects on the autonomic system and then rubs an eye with the same fingers. Occasionally, patients using nebulized bronchodilators for asthma or bronchitis may notice anisocoria when the mask is not well adjusted and some mist reaches one eye. A number of solutions or drugs routinely used to treat dry eyes or allergic conjunctivitis may also induce pharmacologic mydriasis.
Pharmacologic mydriasis from topical agents, such as dilating drops, is usually large(pupil measures at least 7 or 8mm)(▶Fig. 12.35).

The vision is decreased at near (cycloplegia with paralysis of accommodation), and the pupil does not react to light and does not constrict at near. The condition may last up to 10 days if atropine was placed in the eye.
Pharmacologic testing confirms the diagnosis of pharmacologic mydriasis:
1. Place two drops of dilute pilocarpine (0.1%) in both eyes to make sure this is not atonic pupil (in which case, the dilated pupil will constrict because of denervation hypersensitivity, whereas the normal or pharmacologic pupil will not change).
2. If there is no response after 45 minutes, place two drops of pilocarpine 1 or 2% in each eye. The normal pupil will constrict. If the dilated pupil constricts only partially or not at all, the diagnosis of pharmacologic mydriasis is confirmed.
Dysfunction of the Ipsilateral Parasympathetic Pathway
Parasympathetic fibers for pupillary constriction travel along the third cranial nerve to the ipsilateral ciliary ganglion within the orbit. Therefore, third nerve palsies and tonic pupil (Adie pupil) from ciliary ganglion dysfunction may produce a mydriasis with a poorly or nonreactive pupil in response to light.
Tonic Pupil (Adie Pupil)
Tonic pupil is defined as isolated iris sphincter and ciliary muscle dysfunction resulting from damage to the ciliary ganglion or postganglionic short ciliary nerves (in the orbit), followed by aberrant reinnervation.
Clinical symptoms and signs of tonic pupil (▶Fig. 12.36, ▶Fig. 12.37, ▶Fig. 12.38) include the following:
● Large pupil that does not react or reacts poorly to light
● Better constriction when looking at a near target (because the ratio of fibers that serve accommodation compared with pupil constriction is about 30:1, there is an overwhelming amount of regenerating accommodative fibers that respond to a near stimulus but may aberrantly regenerate to the pupil sphincter muscle; this explains the light-near dissociation classically found in a tonic pupil)
● Slow tonic redilation of the pupil from near to distance because of sphincter muscle denervation supersensitivity
● Patients often complain of blurry vision at near (accommodation paralysis) and sensitivity to light (from the large pupil).



Pharmacologic testing confirms the diagnosis of Adie pupil. Dilute pilocarpine can be used to make a pharmacologic diagnosis of tonic pupil (▶Fig. 12.39).
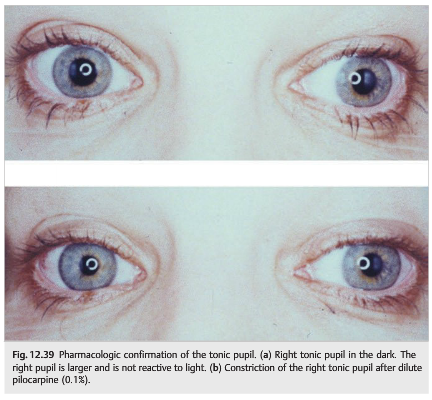
Supersensitivity of denervation makes the tonic pupil sensitive to dilute pilocarpine. Within 5 to 7 days of denervation, cholinergic supersensitivity of the end-organ begins. It is demonstrated by placing two drops of dilute pilocarpine (0.1%) in both eyes. If the iris sphincter has cholinergic supersensitivity, the larger pupil (tonic pupil) becomes smaller than the normal pupil 30 to 45 minutes after instillation of the dilute pilocarpine (the dilute pilocarpine has no effect in the normal eye). Dilute pilocarpine can be made by mixing 0.1mL of 1% pilocarpine with 0.9mL of sterile saline in a 1mL tuberculin syringe.
Causes of tonic pupil include a variety of local processes affecting the ciliary ganglion in the orbit, such as trauma, tumor, ischemia (giant cell arteritis), and infection (viral, e.g., herpes zoster virus or herpes simplex virus, or syphilis). It may happen after laser panretinal photocoagulation and as part of a more widespread autonomic process (diabetes, amyloidosis, and Sjögren syndrome). Adie syndrome is idiopathic in women ages 20 to 40. This syndrome is often characterized by absent lower extremity deep tendon reflexes. It is unilateral in most cases but may become bilateral over years in about 20%of patients.
The evaluation of the patient with a tonic pupil is based mostly on other symptoms or signs, history of trauma or infection, and the patient’s age, and may include blood count, erythrocyte sedimentation rate, C-reactive protein, fasting glucose, hemoglobin A1C, syphilis and human immunodeficiency virus (HIV) testing, and orbital imaging.
Most often, however, confirmation of an Adie pupil with pharmacologic testing, especially in women ages 20 to 60, is satisfactory, and no workup is performed. Over time, tonic pupils tend to become smaller (“little old Adies”). Patients may need reading glasses to correct the accommodation paralysis. Some patients wear tinted glasses because of photophobia. Although dilute pilocarpine corrects the mydriasis and may be used occasionally for cosmetic purposes, its chronic use is not recommended.
Third Nerve Palsy
Mydriasis from isolated third nerve palsy is essentially always associated with an extraocular movement deficit (responsible for diplopia) and/or ptosis (see Chapter 13).
The signs and symptoms of third nerve palsy are ptosis, mydriasis, and abnormal extraocular movements, with impaired adduction, depression, and elevation. Some Patients have incomplete third nerve palsy, but there is always some ptosis and diplopia from mild extraocular muscle deficits (▶Fig. 12.40).

A completely isolated mydriasis is extremely unlikely to be related to a third nerve palsy and should be evaluated clinically and with pharmacologic testing to rule out an Adie pupil or pharmacologic mydriasis prior to obtaining any further workup.
Not all third nerve palsies have pupil involvement. Pupil involvement is common in nuclear, fascicular, and subarachnoid third nerve palsies. Because the pupillary fibers are located superficially, they are vulnerable to compressive processes such as aneurysmal mass effect, various tumors such as pituitary apoplexy, and uncal herniation (▶Fig. 12.41 and ▶Fig. 12.42).
The evaluation of the patient with a third nerve palsy depends on associated symptoms and signs, the pattern of oculomotor nerve involvement, and the age of the patient. The approach to the patient with a third nerve palsy is detailed in Chapter 13.


Pearls
An isolated third nerve palsy with mydriasis may reveal an intracranial aneurysm or pituitary apoplexy, especially if associated with acute headache.
The approach to the patient with anisocoria is detailed in ▶Fig. 12.43.

Fig.12.43 Approach to anisocoria
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.