Questions:
13. Is the visual aura of migraine a hallucination?
14. What is the typical duration of the visual aura episodes of migraine?
15. What are the characteristics of recurrences of the visual aura of migraine?
16. What is the typical duration of the visual phenomenon of occipital seizures?
17. What other neurologic symptoms can migraineurs have?
18. Are migraineurs aware that the images they see are not real?
19. Can migraineurs experience distortion of images?
20. How are occipital seizures frequently described?
21. What are the characteristics of recurrences of occipital seizures?
22. What is peduncular hallucinosis?
23. What lesion is most often related to peduncular hallucinosis?
24. What are the common visual symptoms of narcolepsy?
25. What is the classic tetrad of narcolepsy?
____________________________________________________
Questions with answers:
13. Is the visual aura of migraine a hallucination?
Yes, these visual phenomena are often positive and therefore can be described as hallucinations.
14. What is the typical duration of the visual aura episodes of migraine?
10-30 minutes
15. What are the characteristics of recurrences of the visual aura of migraine?
The visual aura often changes sides and have different patterns.
16. What is the typical duration of the visual phenomenon of occipital seizures?
A few seconds.
17. What other neurologic symptoms can migraineurs have?
Ipsilateral tingling and speech impairment.
18. Are migraineurs aware that the images they see are not real?
Yes
19. Can migraineurs experience distortion of images?
Yes, micropsia and macropsia (Alice in Wonderland syndrome) or tilting of objects can also occur.
20. How are occipital seizures frequently described?
They are described as colorful, positive or negative visual phenomena present in both eyes, including sparkles, pinwheels, bubbles, scotoma, and dots. Although they are often moving, they do not have the stereotyped progression observed in migraine.
21. What are the characteristics of recurrences of occipital seizures?
Often daily with stereotyped visual phenomena for each patient (e.g on the same side).
22. What is peduncular hallucinosis?
It is a rare neurologic syndrome characterized by vivid, usually formed, colorful hallucinations of people, animals, and complex scenes with motion.
23. What lesion is most often related to peduncular hallucinosis?
It is most often related to a midbrain infarction in the region of the peduncle. Patients usually have sleep/wake disorders and are aware that these images are not real. The hallucination usually begins a few days after the lesion occurs and may persist for weeks to months.
24. What are the common visual symptoms of narcolepsy?
Visual hallucinations, described as colorful images, which may involve people, animals, and panoramic scenes. Patients often have a vague sense that someone else is in the room. They also realize that what they are experiencing is not a dream and that they are awake.
25. What is the classic tetrad of narcolepsy?
1. Cataplexy (transient loss of muscle tone)
2. Sleep paralysis (inability to move when the patient first wakes up)
3. Sleep attacks (overwhelming sense of fatigue causing the patient to fall asleep for 10 to 30 minutes)
4. Hypnogogic (entering sleep) and hypnopompic (awakening) hallucinations, lasting several minutes. The hallucinations can be visual, auditory, or tactile.
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
11.3.2 Migraine
Numerous visual phenomena occur during the visual aura of migraine (▶Table 11.1). These visual phenomena are often positive and therefore can be described as hallucinations.

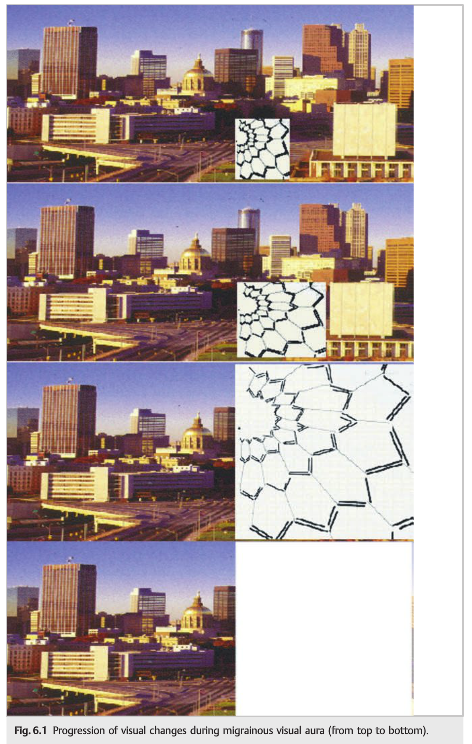
Migrainous visual phenomena usually last between 10 and 30 minutes and progress over time (migrainous march) (see Chapter 6, ▶Fig. 6.1). They may be associated with other neurologic symptoms, such as ipsilateral tingling and speech impairment, and are classically followed by migrainous headaches. Migraineurs are aware that the images they see are not real.
Positive or negative visual phenomena are present in both eyes, either in the entire eye or in one hemifield. Phenomena include phosphenes, which are usually bright or white, and scintillating scotoma, described as progressively enlarging bright scotoma with sharp edges (▶Fig. 11.2). Distortion of images with micropsia and macropsia (Alice in Wonderland syndrome) or tilting of objects can also occur.

11.3.3 Occipital Seizures
Occipital seizures can cause simple and colorful, positive or negative visual phenomena present in both eyes, including sparkles, pinwheels, bubbles, scotoma, and dots. Although they are often moving, they do not have the stereotyped progression observed in migraine. They are short in duration (usually lasting only a few seconds) and may be isolated. They are usually stereotyped for each patient.
Occipital seizures can occur with a variety of occipital lesions or as part of primary occipital seizures, which are more common in children.
11.3.4 Peduncular Hallucinosis
Peduncular hallucinosis is a rare neurologic syndrome characterized by vivid, usually well-formed, colorful hallucinations of people, animals, and complex scenes with motion. It is most often related to a midbrain infarction in the region of the peduncle, and is also likely a “release phenomenon” (▶Fig. 11.3).
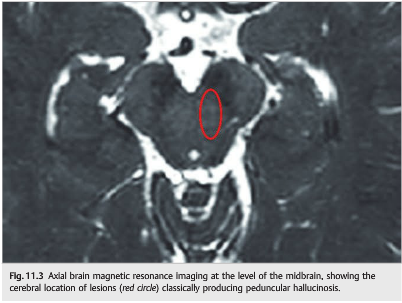
Patients usually have sleep/wake disorders and are aware that these images are not real. The hallucination usually begins a few days after the lesion occurs and may persist for weeks to months.
11.3.5 Narcolepsy
Visual hallucinations are a common presenting complaint of narcolepsy. They are described as colorful images, which may involve people, animals, and panoramic scenes.
Patients often have a vague sense that someone else is in the room. They also realize that what they’re experiencing is not a dream and that they are awake.
The classic tetrad of narcolepsy includes the following:
● Cataplexy (transient loss of muscle tone)
● Sleep paralysis (inability to move when the patient first wakes up)
● Sleep attacks (overwhelming sense of fatigue causing the patient to fall asleep for 10to 30minutes)
● Hypnogogic (entering sleep) and hypnopompic (awakening) hallucinations, lasting several minutes. The hallucinations can be visual, auditory, or tactile.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.