Questions:
1. What is the role of the inferior (ventral) or occipitotemporal pathway?
2. What is the role of the superior (dorsal) or occipitoparietal pathway?
3. What is alexia without agraphia?
4. How does one test for alexia without agraphia?
5. Where is the lesion in alexia without agraphia?
6. What clinical finding is associated with alexia without agraphia
____________________________________________________
Questions with answers:
1. What is the role of the inferior (ventral) or occipitotemporal pathway?
The inferior (ventral) or occipitotemporal pathway for object recognition is the what pathway. It extends from below the calcarine fissure into the adjacent temporal lobe. It facilitates object recognition and color perception. Disorders here include achromatopsia, prosopagnosia, alexia, and topographagnosia.
2. What is the role of the superior (dorsal) or occipitoparietal pathway?
The superior (dorsal) or occipitoparietal pathway for object localization is the where pathway. It extends from the upper bank of the calcarine fissure and into the adjacent parietal lobe. It processes visuospatial attributes, including location and motion. Disorders here include akinetopsia, Balint syndrome (simultagnosia, ocular apraxia, and optic ataxia), and hemineglect.
3. What is alexia without agraphia?
It is the Higher Cortical Disorder in which the patient is able to write but not read.
4. How does one test for alexia without agraphia?
Have the patient try to read a text and then tell the patient some words to write and determine if the patient wrote those words correctly.
5. Where is the lesion in alexia without agraphia?
Left occipital lobe and splenium of the corpus callosum
6. What clinical finding is associated with alexia without agraphia?
Right homonymous hemianopia
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
10 Disorders of Higher Cortical Function
Unlike the anterior visual and geniculocalcarine pathways that deliver basic visual information from the eyes to the occipital cortex, association cortical visual areas (higher cortical areas) perform the more complex interpretation of visual information. Many of the syndromes of higher cortical dysfunction are secondary to a disconnection of the flow of visual information between the striate cortex and other cortical regions. When these areas are damaged, visual processing is abnormal despite often normal visual acuity and visual fields.
This chapter focuses on some of the main visual disorders of higher cortical function, particularly their clinical and radiologic findings and causes, commonly encountered in neuro-ophthalmology.
10.1 Classification
Disorders of higher cortical function are often grouped into two processing streams. The first stream, the inferior (ventral) or occipitotemporal pathway for object recognition, extends from below the calcarine fissure into the adjacent temporal lobe. It facilitates object recognition and color perception. Disorders here include achromatopsia, prosopagnosia, alexia, and topographagnosia.
The second stream, the superior (dorsal) or occipitoparietal pathway for object localization extends from the upper bank of the calcarine fissure into the adjacent parietal lobe. It processes visuospatial attributes, including location and motion. Disorders here include akinetopsia, Balint syndrome (simultagnosia, ocular apraxia, and optic ataxia), and hemineglect.
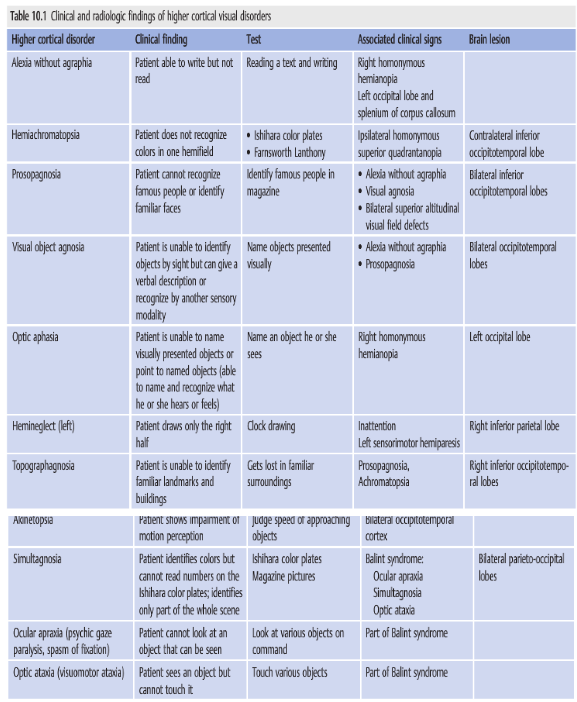
▶Table 10.1 lists the clinical findings, recommended tests, associated clinical signs, and lesions associated with these higher cortical disorders.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.