Questions:
95. Do anterior and large intraorbital lesions produce optic disc swelling?
96. Do intracranial, intracanalicular, and posterior orbital compressive lesions typically produce disc swelling?
97. How is the presumed diagnosis of compressive optic neuropathy confirmed?
98. What are the characteristic findings of optic nerve sheath meningioma?
99. What are 7 characteristic findings of optic nerve glioma/pilocytic astrocytoma?
100. What are 6 characteristic findings of craniopharyngioma?
____________________________________________________
Questions with answers:
95. Do anterior and large intraorbital lesions produce optic disc swelling?
Yes, anterior and large intraorbital lesions often produce optic disc swelling.
96. Do intracranial, intracanalicular, and posterior orbital compressive lesions typically produce disc swelling?
No.
97. How is the presumed diagnosis of compressive optic neuropathy confirmed?
The diagnosis of compressive optic neuropathy is confirmed by imaging. However, tumors compressing the anterior visual pathways may be missed on routine brain CT or MRI. Dedicated views of the orbits, the sella turcica, and the cavernous sinus are necessary and should be obtained based on clinical suspicion. MRI with thin sections, contrast and fat suppression are recommended.
98. What are the characteristic findings of optic nerve sheath meningioma
1. It occurs more often in women.
2. There is slowly progressive monocular visual loss.
3. Monocular transient vision loss is common.
4. Physical findings include disc pallor or edema, optociliary shunts and the tram-track sign on neuroimaging.
99. What are 7 characteristic findings of optic nerve glioma/pilocytic astrocytoma?
1. age < 10
2. progressive visual loss
3. proptosis
4. strabismus
5. nystagmus in young children
6. neuroimaging demonstrates a fusiform enlargement of the optic nerve and often chiasmal involvement.
7. Neurofibromatosis type I is present in 30%.
100. What are 6 characteristic findings of craniopharyngioma?
1. two age ranges ( age <20, and age 50–70)
2. progressive bitemporal or homonymous VF defect
3. headache
4. hydrocephalus
5. papilledema
6. endocrine dysfunction
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
8.6 Compressive and Infiltrative Optic Neuropathies
Various lesions may compress or infiltrate the intraorbital, intracranial, or prechiasmal optic nerves. Anterior or large intraorbital lesions often produce optic disc swelling (▶Fig. 8.26), whereas intracranial, intracanalicular, and posterior orbital compressive lesions typically do not produce disc swelling.


8.6.1 Characteristics
The clinical presentation varies based on the type and location of the mass:
● Progressive unilateral optic neuropathy (progressive visual loss with abnormal color vision, visual field defect, and optic disc pallor or disc edema)
● Intracranial lesions in the region of the chiasm that may produce vision loss in both eyes (bilateral optic neuropathies, bitemporal hemianopia, junctional scotoma)
● Usually, no pain with eye movements
● Headache if raised intracranial pressure (large tumor, hydrocephalus) or involvement of branches of the trigeminal nerve (cavernous sinus)
● Proptosis and diplopia common in orbital lesions
● Cranial nerve palsies common in lesions extending into the cavernous sinus
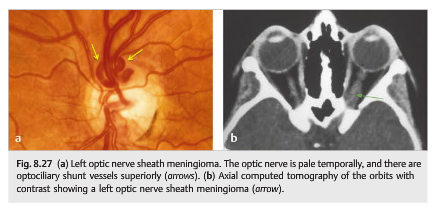
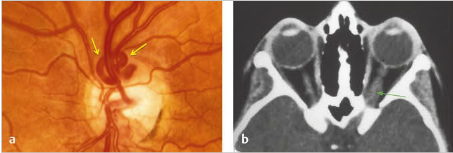
Optociliary shunt vessels may develop as a result of optic nerve compression(▶Fig. 8.27).
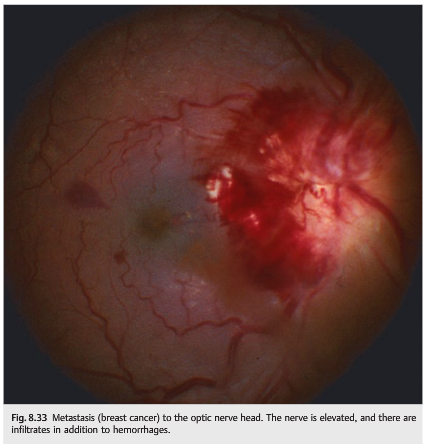
The optic nerve may also be compressed or infiltrated by neoplasm (▶Fig. 8.28,▶Fig. 8.29, ▶Fig. 8.30, ▶Fig. 8.31, ▶Fig. 8.32, ▶Fig. 8.33, ▶Fig. 8.34, ▶Fig. 8.35) or by an inflammatory process, such as orbital inflammatory pseudotumor or thyroid eye disease (see ▶Fig. 8.31).






Cupping of the optic nerves is not uncommon in chronic compression. There is pallor of the remaining rim, unlike in glaucomatous nerve cupping, in which the cups are large with retained pink rims (▶Fig. 8.30).
8.6.2 Causes
Causes of compressive optic neuropathy include the following:
● Neoplastic
○ Optic nerve sheath meningioma
○ Intraorbital tumor (hemangioma, lymphangioma, metastasis, etc.)
○ Sphenoid meningioma
○ Pituitary tumor
○ Craniopharyngioma
● Non-neoplastic
○ Thyroid eye disease
○ Orbital pseudotumor
○ Orbital hemorrhage
○ Paget disease
○ Fibrous dysplasia
○ Ophthalmic artery aneurysm
○ Ectatic internal carotid artery
Causes of infiltrative optic neuropathy (▶Table 8.4):
● Neoplastic○ Optic nerve glioma
○ Metastatic carcinoma
○ Nasopharyngeal carcinoma and other contiguous tumors
○ Lymphoma○ Leukemia
○ Meningeal carcinomatosis
● Non-neoplastic
○ Sarcoidosis


Pearls
The diagnosis of compressive optic neuropathy is confirmed by imaging. However, tumors compressing the anterior visual pathways may be missed on routine brain CT or MRI. Dedicated views of the orbits, the sella turcica, or the cavernous sinus are necessary and should be obtained based on clinical suspicion. MRI with contrast is preferred.
8.6.3 Diagnosis
In most cases, a presumed diagnosis of compressive or infiltrative optic neuropathy is made based on clinical presentation and neuroimaging. A biopsy is the only way to obtain a definite diagnosis, but it is rarely possible in optic nerve tumors or optic nerve sheath meningiomas because optic nerve biopsy usually results in permanent visual loss. In many of these cases, treatment is based on the presumed diagnosis.
Optic nerve sheath meningiomas arise from the dural sheath of the intraorbital optic nerve. This tumor occurs mostly in middle-aged women who present with unilateral, painless, progressive loss of vision in one eye. Episodes of transient monocular visual loss are common. The optic disc is often already pale at the time of diagnosis, and it may be swollen. There may be optociliary shunt vessels on the optic disc (dilated veins resulting from chronic central retinal vein compression) (Fig. 8.27).
Fig.8.27 (a) Left optic nerve sheath meningioma. The optic nerve is pale temporally, and there are optociliary shunt vessels superiorly (arrows). (b) Axial computed tomography of the orbits with contrast showing a left optic nerve sheath meningioma (arrow).
Imaging often misses optic nerve sheath meningiomas, which can be difficult to visualize, especially if there are no dedicated orbital images with fat suppression and contrast. Without treatment, the vision deteriorates, and the tumor may even extend intracranially through the optic canal. However, its progression is very slow, and treatment is based on the amount of visual loss and the size of the tumor. Prognosis is mostly based on the type and location of the tumor, as well as the duration of visual loss. Vision often improves (at least partially) after treatment.
Pilocytic astrocytoma and optic nerve glioma are more common and more benign in children than in adults.
Pituitary tumors are the most common cause of compressive optic neuropathy.
Pearls
Low-tension glaucoma is a rare type of glaucoma in which patients with normal intraocular pressure develop a glaucomatous optic neuropathy. It is a diagnosis of exclusion, and other causes of optic neuropathies, particularly compressive, need to be ruled out by neuroimaging
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.