Questions:
20. Radiation retinopathy a chronic, painless, progressive retinal vasculopathy. True or False?
21. Radiation retinopathy may be unilateral or bilateral and occur months or years after radiotherapy. True or False?
22. Radiation retinopathy is more common in patients with underlying retinal vascular disease (e.g., hypertension or diabetes). True or False?
23. What are 5 key findings of radiation retinopathy?
24. What are 6 complications of radiation retinopathy?
25. What is the chief feature of Purtscher retinopathy?
26. What is the significance of bilateral retinal vascular tortuosity?
27. What are 2 retinal vascular malformations?
____________________________________________________
Questions with answers:
20. Is radiation retinopathy a chronic, painless, progressive retinal vasculopathy?
True
21. Radiation retinopathy may be unilateral or bilateral and occur months or years after radiotherapy. True or False?
True
22. Radiation retinopathy is more common in patients with underlying retinal vascular disease (e.g., hypertension or diabetes). True or False?
True
23. What are 5 key findings of radiation retinopathy?
1. Retinal hemorrhages
2. Retinal microaneurysms
3. Retinal exudates
4. Cotton wool spots
5. Macular edema
24. What are 6 complications of radiation retinopathy
1. retinal ischemia
2. retinal neovascularization
3. vitreous hemorrhage
4. traction retinal detachment
5. neovascularization of the anterior segment
6. optic atrophy
25. What is the chief feature of Purtscher retinopathy?
The chief feature of Purtscher retinopathy is bilateral peripapillary retinal infarctions with numerous cotton wool spots. This type of retinopathy classically occurs after trauma, acute pancreatic disorders, and amniotic fluid embolism.
26. What is the significance of bilateral retinal vascular tortuosity?
It is usually asymptomatic and discovered during a routine funduscopic examination. It is rarely associated with retinal hemorrhages and cerebral leukoencephalopathy. It may be familial.
27. What are 2 retinal vascular malformations?
Cavernous hemangioma & Retinal hemangioma
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
7.7 Radiation Retinopathy
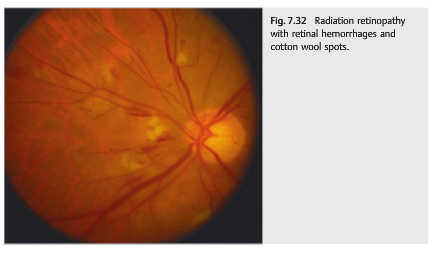
Radiation retinopathy is a chronic progressive retinal vasculopathy induced by radiation and responsible for progressive, painless visual loss (▶Fig. 7.32).
Radiation retinopathy may be unilateral or bilateral, depending on the type of radiation. It develops months or years after radiotherapy and is more common in patients with underlying retinal vascular disease (e.g., hypertension or diabetes).
Key findings include the following:
● Retinal hemorrhages
● Retinal microaneurysms
● Retinal exudates
● Cotton wool spots
● Macular edema
Complications of radiation retinopathy include retinal ischemia, retinal neovascularization, vitreous hemorrhage, traction retinal detachment, neovascularization of the anterior segment, and optic atrophy.
7.8 Purtscher Retinopathy
The chief feature of Purtscher retinopathy is bilateral peripapillary retinal infarctions with numerous cotton wool spots (▶Fig. 7.33).
This type of retinopathy classically occurs after trauma, acute pancreatic disorders, and amniotic fluid embolism.

7.9 Retinal Vascular Tortuosity
Retinal vascular tortuosity (▶Fig. 7.34) is bilateral, involving the arteries and veins. Itis usually asymptomatic and can be discovered during a routine funduscopic examination.
It is rarely associated with retinal hemorrhages and cerebral leukoencephalopathy. It may be familial.

7.10 Retinal Vascular Malformations
Retinal vascular malformations are usually found during a routine fundus examination (▶Fig. 7.35 and ▶Fig. 7.36).


Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.