Questions:
12. What may develop in patients with severe stenosis or occlusion of the ipsilateral common carotid artery or internal carotid artery and poor collateral circulation?
13. What condition should venous stasis retinopathy, or hypotensive retinopathy, suggest?
14. What are the symptoms of the ocular ischemic syndrome?
15. What are signs of the ocular ischemic syndrome?
16. What is the prognosis of the ocular ischemic syndrome?
17. What should be ruled out in a patient who has a rapidly worsening ocular ischemic syndrome?
18. What should be checked in all patients with headache and bilateral optic nerve swelling?
19. What 10 classic systemic disorders associated with retinal vasculitis?
____________________________________________________
Questions with answers:
12. What may develop in patients with severe stenosis or occlusion of the ipsilateral common carotid artery or internal carotid artery and poor collateral circulation?
Ocular ischemia may develop in patients with severe stenosis or occlusion of the ipsilateral internal carotid artery and poor collateral circulation. These patients often have low blood flow in the ophthalmic artery. The flow is sometimes reversed in the ophthalmic artery to protect the ipsilateral brain, producing a “steal phenomenon” involving the eye.
13. What condition should venous stasis retinopathy, or hypotensive retinopathy, suggest?
These can be is often the first sign of chronic ocular ischemia.
14. What are the symptoms of the ocular ischemic syndrome?
Patients may be asymptomatic, have episodes of hemodynamic transient monocular visual loss when standing up, after a meal, or with exposure to bright lights. The patients may experience dull periocular pain that may only be present when the patient is standing. There may be visual acuity loss and changes in the visual field.
15. What are signs of the ocular ischemic syndrome?
Venous stasis retinopathy or hypotensive retinopathy is the first sign of chronic ocular ischemia. It resembles diabetic retinopathy or central retinal vein occlusion and is characterized by a unilateral appearance, dilation, and tortuosity of the retinal veins, and blot hemorrhages, mostly in the midperiphery of the retina. Neovascularization may develop involving the retina and the anterior segment. It results in neovascular glaucoma (increased intraocular pressure), atonic iris (dilated and nonreactive pupil), cataract, or corneal edema.
16. What is the prognosis of the ocular ischemic syndrome?
The prognosis of the ocular ischemic syndrome is poor. Laser panretinal photocoagulation of the ischemic retina may reduce neovascularization.
17. What should be ruled out in a patient who has a rapidly worsening ocular ischemic syndrome?
Giant cell arteritis may be the cause in an elderly patient with rapidly worsening ocular ischemic syndrome.
18. What should be checked in all patients with headache and bilateral optic nerve swelling?
The blood pressure needs to be measured in all patients with bilateral optic nerve edema. Acutely elevated systemic arterial blood pressure (malignant hypertension) may present with bilateral optic nerve edema and headaches. Retinal changes may be absent.
19. What 10 classic systemic disorders associated with retinal vasculitis?
1. Syphilis
2. Cytomegalovirus
3. Toxoplasmosis
4. Cat scratch disease
5. Herpes simplex
6. Herpes zoster
7. Sarcoidosis
8. Systemic lupus erythematosus
9. Behçet syndrome
10. Multiple sclerosis (peripheral periphlebitis)
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
7.2 Ocular Ischemic Syndrome
Chronic hypoperfusion of the eye results in diffuse ocular ischemia. Ocular ischemia develops in patients with severe stenosis or occlusion of the ipsilateral internal carotid artery and poor collateral circulation. These patients often have low blood flow in the ophthalmic artery. The flow is sometimes reversed in the ophthalmic artery to protect the ipsilateral brain (there is then a steal phenomenon involving the eye) (see Chapter 6, ▶Fig. 6.15 and ▶Fig. 6.16).
7.2.1 Features
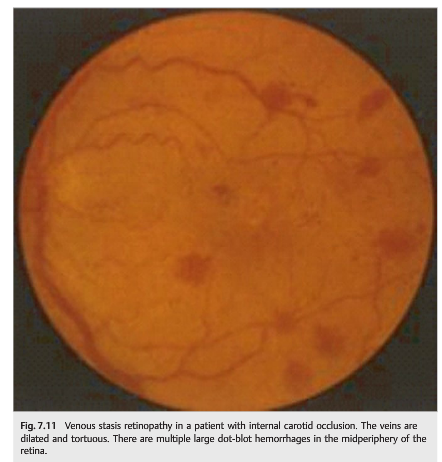
Venous stasis retinopathy (▶Fig. 7.11), or hypotensive retinopathy, is the first sign of chronic ocular ischemia. It resembles diabetic retinopathy or central retinal vein occlusion and is characterized by a unilateral appearance, dilation and tortuosity of the retinal veins, and blot hemorrhages, mostly in the midperiphery of the retina.
Venous stasis retinopathy is usually asymptomatic. Patients may have episodes of hemodynamic transient monocular visual loss when standing up, after a meal, or with exposure to bright lights.
Other features of ocular ischemic syndrome are dull periocular pain that is present when the patient is standing up (it resolves when the patient is lying down), episcleral arteries that may be dilated (result from collateral circulation to the eye from branches of the external carotid artery), low intraocular pressure, and pseudointraocular inflammation.
Neovascularization may develop involving the retina and the anterior segment. It results in neovascular glaucoma (increased intraocular pressure), atonic iris (dilated and nonreactive pupil), cataract, or corneal edema.
7.2.2 Treatment and Prognosis
At this stage, revascularization of the eye (e.g., by performing a carotid endarterectomy if there is an ipsilateral internal carotid artery stenosis) may result in improvement of the retinopathy. If the eye is not revascularized, ocular ischemic syndrome develops (▶Fig. 7.12).
The prognosis of ocular ischemic syndrome is poor.
Laser panretinal photocoagulation of the ischemic retina may reduce neovascularization (e.g., as for proliferative diabetic retinopathy). These patients often have ipsilateral internal carotid occlusion, however, and revascularization is not always possible (extra-intracranial bypass procedure is sometimes indicated). Even when revascularization of the eye is performed, the visual prognosis remains poor.

Pearls
Look for giant cell arteritis in the elderly patient with rapidly worsening ocular ischemic syndrome. Giant cell arteritis involves branches of the external carotid artery, which usually supply most of the eye via collateral circulation when there is an internal carotid occlusion. Any disorder affecting branches of the external carotid artery (e.g., giant cell arteritis) will compromise the collateral circulation and may precipitate acute ocular ischemia.
7.3 Retinal Vein Occlusion
7.3.1 Features
Central and branch retinal vein occlusions (▶Fig. 7.13, ▶Fig. 7.14, ▶Fig. 7.15) produce subacute monocular visual loss. The loss of vision is often progressive over a few days and is secondary largely to macular edema and macular ischemia. Relatively prolonged (up to 30 minutes) episodes of transient monocular visual loss may occur before permanent visual loss (see Chapter 6, ▶Fig. 6.17).


7.3.2 Types of Retinal Vein Occlusions
Acute Central Retinal Vein Occlusion
Acute central retinal vein occlusion is characterized by painless monocular loss of vision over a few hours or a few days; dilated, tortuous veins; retinal hemorrhages; and retinal and optic nerve edema. Retinal ischemia and cotton wool spots suggest an ischemic form. A RAPD is seen if there is extensive retinal ischemia (poor prognosis). Acute central retinal vein occlusion may present with isolated optic nerve edema (▶Fig. 7.16).
These patients are often mistaken as having an acute optic neuropathy, such as anterior ischemic optic neuropathy.
The usual presence of retinal hemorrhages distant from the swollen optic nerve suggests central retinal vein occlusion. Fluorescein angiography is useful to differentiate vein occlusion from other causes of disc edema.

▶Table 7.3 lists the causes of acute retinal vein ischemia, with suggested tests.

Acute Branch Retinal Vein Occlusion and Hemiretinal Vein Occlusion
Both acute branch retinal vein occlusion and hemiretinal vein occlusion are characterized by painless monocular loss of vision over a few hours or a few days; dilated, tortuous veins; and retinal hemorrhages with edema in the territory of the occluded vein (see ▶Fig. 7.14 and ▶Fig. 7.15).


7.3.3 Natural History and Patient Evaluation
Most retinal vein occlusions occur in patients older than age 50 who have vascular risk factors. In these cases, vascular risk factors need to be aggressively controlled, but very little workup is obtained. Blood tests looking for hypercoagulable states are obtained only in patients in whom there is a high suspicion of hypercoagulability (recurrent retinal vein occlusions, bilateral retinal vein occlusion, young patients, and/or a personal or familial history of vein occlusions) (see Chapter 20).
Orbital imaging is obtained only in patients with clinical evidence of orbital syndrome, cavernous sinus syndrome, or optic neuropathy.
7.3.4 Prognosis and Treatment
The visual prognosis is mostly based on the type of vein occlusion (ischemic form or not). When visual loss is mostly related to macular edema, vision usually improves over time. When the macula is ischemic (there is a RAPD in the affected eye), the visual prognosis is poor. In most cases, the hemorrhages and retinal edema resolve spontaneously over a few weeks or months. In nonischemic central retinal vein occlusion, the visual prognosis is good, and visual function improves when macular edema resolves. Ischemic forms have a high risk of ocular neovascularization and permanent visual loss. Various treatments, such as decreasing intraocular pressure, retinal laser, intravitreal injections of steroids, and anti–vascular endothelial growth factor (VEGF) drugs, are ordered by retinal specialists.
Shunt vessels may develop after a central retinal vein occlusion (▶Fig. 7.17).
It is common to observe these dilated vessels during a routine ocular examination. An optic nerve sheath meningioma needs to be ruled out by an MRI scan of the orbits with contrast and fat suppression.

7.4 Diabetic Retinopathy
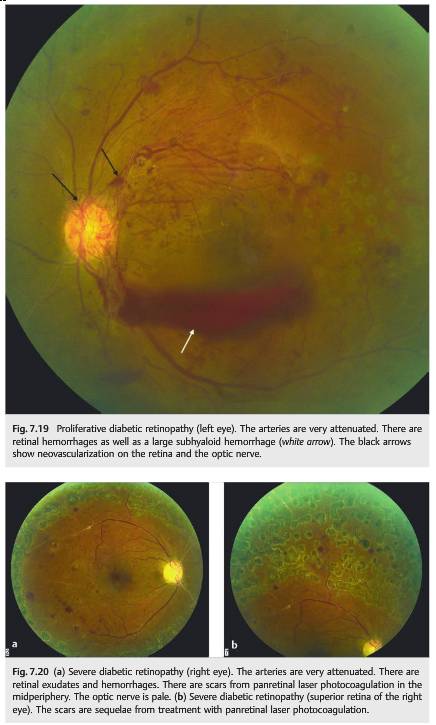
Diabetic retinopathy (▶Fig. 7.18, ▶Fig. 7.19, and ▶Fig. 7.20) is a common cause of visual loss. Macular edema and retinal ischemia can result in severe visual loss.
The ischemia is diffuse, often involves the macula (responsible for central visual loss), and is ultimately complicated by neovascularization of the eye (proliferative diabetic retinopathy).
The neovascularization in proliferative diabetic retinopathy is responsible for hemorrhages and traction retinal detachment. Destruction of the peripheral retina with laser (panretinal photocoagulation) decreases the neovascularization but also results in night blindness and constriction of the visual field.

7.5 Hypertensive Retinopathy
Retinal vascular changes occur as a result of chronically elevated arterial blood pressure, usually bilaterally. Hypertensive retinopathy (▶Fig. 7.21, ▶Fig. 7.22, and ▶Fig. 7.23) is associated with a higher risk of cardiovascular disease, including coronary artery disease and stroke. It is a marker of poorly controlled arterial hypertension.

7.5.1 Features
The following are key features of hypertensive retinopathy:
● Bilateral retinal vascular changes (may be asymmetric)
● Narrowing and irregularity of retinal arteries
● Arteriovenous nicking (narrowing of retinal veins at arteriovenous crossing sites)
● Retinal hemorrhages
● Microaneurysms
● Cotton wool spots
Moderate chronic hypertensive retinopathy is usually asymptomatic. Visual loss may occur as a result of macular exudates, macular edema, and chronic retinal ischemia.
Pearls
The blood pressure needs to be measured in all patients with bilateral optic nerve edema. Acutely elevated systemic arterial blood pressure may present with bilateral optic nerve edema and headaches. Retinal changes may be absent.
Acute hypertensive retinopathy (▶Fig. 7.24 and ▶Fig. 7.25) represents retinal and choroidal vascular changes occurring as a result of acutely elevated systemic arterial blood pressure.
Key features of acute hypertensive retinopathy are as follows:
● Retinal arteriolar spasm
● Retinal hemorrhages
● Cotton wool spots
● Retinal exudates
● Serous retinal detachment
● Optic nerve edema
Acute hypertensive retinopathy is often complicated by permanent visual loss from choroidal ischemia, retinal pigment epithelium changes, and ischemic optic neuropathy. Other complications are bilateral visual loss from cerebral blindness (reversible posterior leukoencephalopathy), intracranial hemorrhages, and renal failure.


7.6 Retinal Vasculitis
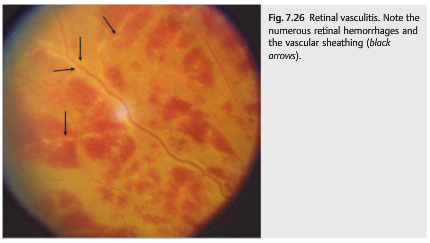
Vasculitis of the retinal vasculature (▶Fig. 7.26 and ▶Fig. 7.27) can involve the arteries, the veins, or both, and may result in visual loss. As for cerebral vasculitis, the term retinal vasculitis implies that there is inflammation in or around the vessel wall. It therefore should be reserved for those disorders definitely secondary to inflammation. For example, Susac syndrome is associated with retinal vasculopathy, not vasculitis—there is no inflammation despite the fluorescein angiographic vascular leakage.

Causes of retinal vasculitis are numerous and include all classic causes of cerebral and systemic vasculitides (see Chapter 20). Recognition of whether the vasculitis involves the arteries or the veins, and associated ocular findings, is helpful.
For example, retinal vasculitis from Behçet syndrome involves the veins, is usually extensive, and is classically associated with anterior chamber inflammation. Periphlebitis associated with multiple sclerosis involves only the veins, affects the peripheral retina, and is asymptomatic. The involved vessels are attenuated (appear small), with sheathing (whitish line along the vessels), and are sometimes occluded (▶Fig. 7.28).

There are retinal hemorrhages and cotton wool spots secondary to retinal ischemia. Fluorescein angiography demonstrates occlusion of the small vessels and leakage of fluorescein (▶Fig. 7.29).

Retinal vasculitis may be localized and mild. Finding vascular sheathing in an area of retinal ischemia is highly suggestive of vasculitis. The following classic systemic disorders are associated with retinal vasculitis:
● Infections
○ Syphilis
○ Cytomegalovirus (▶Fig. 7.30)
○ Toxoplasmosis
○ Cat scratch disease
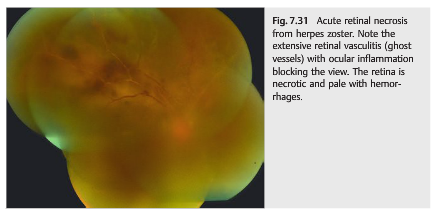
○ Herpes simplex and herpes zoster (▶Fig. 7.31)

● Inflammatory disorders
○ Sarcoidosis
○ Systemic lupus erythematosus
○ Behçet syndrome ○ Multiple sclerosis (peripheral periphlebitis) (see ▶Fig. 7.28)
Reference: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.