Questions:
10. What provides the blood supply to the anterior cerebral hemispheres and to the eyes?
11. What is the blood supply to the occipital lobes?
12. What finding does occlusion of a posterior cerebral artery produce?
13. A patient complains of loss of visual field in one eye, what should be ruled-out on examination?
14. What 5 mechanisms should be considered in the differential diagnosis of transient monocular visual loss?
15. What is the most likely cause of transient visual obscurations (brief blackouts or grey-outs) on change of posture?
16. What is the likely cause of gaze-evoked episodes of transient monocular vision loss?
17. Which ocular diagnoses involving the anterior segment of the eye should be considered when a patient complains of transient monocular blurring of vision?
18. How long does the transient loss of vision last when the cause is retinal emboli?
19. What is the typical length of time of transient monocular vision loss in optic nerve head anomalies?
20. What should be considered in a patient who has eye or brow pain with transient monocular vision loss?
21. What should be considered in a patient who has transient monocular vision loss and neck pain or ipsilateral Horner syndrome?
22. What should be considered in a patient who has transient monocular vision loss and simultaneous contralateral hemisensory or motor findings?
23. What should be considered in a patient who has transient monocular vision loss and presyncope?
24. Will the transient monocular vision loss due to carotid occlusive disease be partial vision loss or complete vision loss?
25. What is the major source of collateral circulation to the eye?
26. What are 5 vascular mechanisms of transient monocular visual loss?
27. Should the presence of emboli in the eye found on a routine exam prompt a workup for their source?
28. How long does the monocular visual loss from spasm of the central retinal artery last?
__________________________________________
Questions with answers:
10. What provides the blood supply to the anterior cerebral hemispheres and to the eyes?
Internal carotid arteries
11. What is the blood supply to the occipital lobes?
The posterior cerebral arteries (PCA), which originate from the basilar artery are the primary source. The tip of the occipital lobe, where the macular (central) homonymous hemifields are represented, often has a dual blood supply from terminal branches of the PCA and of the middle cerebral artery (MCA).
12. What finding does occlusion of a posterior cerebral artery produce?
Contralateral homonymous hemianopia
13. A patient complains of loss of visual field in one eye, what should be ruled-out on examination?
When patients identify a field defect as being from one eye, a homonymous hemianopsia is often found.
14. What 5 mechanisms should be considered in the differential diagnosis of transient monocular visual loss?
1. Transient eye surface disease (Dry eye)
2. Vascular
3. Acute angle closure glaucoma
4. Optic nerve head anomalies/problems
5. Orbital mass lesion
15. What is the most likely cause of transient visual obscurations (brief blackouts or grey-outs) on change of posture?
This usually indicates underlying optic nerve head edema or optic nerve anomalies causing high tissue pressure at the optic nerve head. Although disc edema results from a variety of disorders, the most likely cause of posture related transient visual obscuration is papilledema.
16. What is the likely cause of gaze-evoked episodes of transient monocular vision loss?
An orbital mass
17. Which ocular diagnoses involving the anterior segment of the eye should be considered when a patient complains of transient monocular blurring of vision?
Ocular diseases involving the anterior segment of the eye that can cause TMVL include dry eyes, keratoconus, hyphema, and angle closure glaucoma. Retinal Detachment can also rarely produce transient visual loss.
18. How long does the transient loss of vision last when the cause is retinal emboli?
One to four minutes
19. What is the typical length of time of transient monocular vision loss in optic nerve head anomalies?
Very brief, a few seconds and may be precipitated by bending over or Valsalva maneuvers.
20. What should be considered in a patient who has eye or brow pain with transient monocular vision loss?
Angle closure glaucoma and cranial arteritis
21. What should be considered in a patient who has transient monocular vision loss and neck pain or ipsilateral Horner syndrome?
Cervical carotid artery dissection
22. What should be considered in a patient who has transient monocular vision loss and simultaneous contralateral hemisensory or motor findings?
Ipsilateral carotid artery stenosis
23. What should be considered in a patient who has transient monocular vision loss and presyncope?
Hypotension or hyperviscosity syndrome
24. Will the transient monocular vision loss due to carotid occlusive disease be partial vision loss or complete vision loss?
Either
25. What is the major source of collateral circulation to the eye?
The external carotid artery
26. What are 5 vascular mechanisms of transient monocular visual loss?
1. emboli
2. hypoperfusion/ischemia of the eye
3. vasculitis
4. arterial vasospasm
5. venous congestion
27. Should the presence of emboli in the eye found on a routine exam prompt a workup for their source?
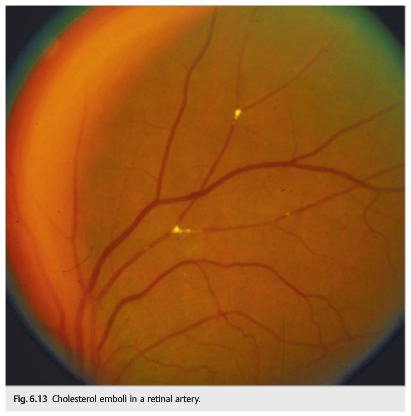
Yes. Asymptomatic retinal emboli (most often cholesterol) are found in 1 to 2% of patients older than age 50. The common and internal carotid arteries are the most common sources of retinal cholesterol emboli. A prompt carotid ultrasound and an evaluation for atheromatous vascular risk factors should be obtained. Vascular risk factors need to be aggressively controlled. Retinal cholesterol emboli increase the risk of cardiac disease therefore also warranting a cardiac evaluation.
28. How long does the monocular visual loss from spasm of the central retinal artery last?
Vasospasm of the central retinal artery may produce episodes of isolated, painless, sudden, complete loss of vision in one eye, usually lasting between 30 seconds and 1 minute. Vasospasm most often affects young, healthy people, and its cause is unclear. The prognosis is excellent without subsequent risk of ocular or cerebral infarction. Antiplatelet agents or calcium channel inhibitors are usually prescribed.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
6.2.1 Differential Diagnosis
TMVL can be vascular (transient ischemia in the territories of the ophthalmic artery, central retinal artery and its branches, posterior ciliary arteries, or central retinal vein), can be ocular in origin (such as from dry eyes or attacks of angle closure glaucoma), or can result from optic nerve head anomalies.
An orbital mass may produce gaze-evoked episodes of TMVL. The examination may be normal between episodes when the mass is relatively small. Movements of the eye result in stretching of the optic nerve and intermittent compression of the nerve or of its blood supply, with resulting transient loss of vision.
Eyes with a narrow anterior chamber angle may have episodes of angle closure glaucoma resolving spontaneously. During such episodes, the intraocular pressure is elevated, and patients complain of painful transient monocular blurry vision with the perception of halos around lights.
Patients with dry eyes often complain of fluctuation of vision, especially while reading.
Pearls
Transient visual obscurations (TVOs) are characterized by brief blackouts or “gray-outs” of vision and are precipitated by changes in posture, such as bending over. They usually indicate underlying optic nerve head edema or optic nerve anomalies causing high tissue pressure at the optic nerve head. Although disc edema results from a variety of disorders, the most likely cause of TVOs is papilledema from raised intracranial pressure.
6.2.2 Patient Evaluation
The clinical history and a detailed ocular examination help determine the mechanism of the TMVL.
Among the first things to ask the patient about are the onset and duration of TMVL. The answers can help determine the cause. For example, retinal emboli produce a very sudden TMVL, lasting from 1 to 4 minutes. TMVL as a result of ocular hypoperfusion would be progressive, at least 5 to 10 minutes, and be precipitated by standing up or looking at bright lights. Venous congestion causes a progressive loss, lasting at least 10 to 20 minutes. TVOs from optic nerve head anomalies are very brief, lasting only a few seconds, and are precipitated by bending over or by Valsalva maneuvers.
Accompanying manifestations helpful in determining the mechanism of TMVL include the following:
● Headache, scalp tenderness, jaw claudication, and diplopia: giant cell arteritis
● Eye or brow pain: intermittent angle closure glaucoma or giant cell arteritis
● Neck pain: cervical carotid artery dissection
● Ipsilateral Horner syndrome: carotid artery dissection
● Simultaneous contralateral hemisensory or motor findings: ipsilateral carotid artery stenosis
● Presyncope: systemic hypotension or a hyperviscosity syndrome
● TMVL when moving the eye: orbital mass
● Blurry vision when reading: dry eyes
The ocular examination can help to rule out local causes of TMVL and detect retinal emboli, retinal ischemia, venous stasis retinopathy, or evidence of optic nerve ischemia.
Eyes with a narrow anterior chamber angle may have episodes of angle closure glaucoma resolving spontaneously (▶Fig. 6.5).
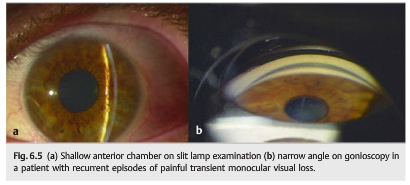
During such episodes, the intraocular pressure is elevated, and patients complain of painful transient monocular blurry vision with the perception of halos around lights.
6.2.3 Vascular TMVL
Vascular TMVL is the most common and perhaps most important ophthalmologic symptom of carotid occlusive disease (see Chapter 20). Patients with vascular TMVL complain of isolated or recurrent episodes of acute, monocular loss of vision that may be partial or complete.
▶Fig. 6.6 shows the blood supply of the eyes and the orbits.

The main blood supply to the eye and orbital contents comes from the ophthalmic artery, a branch of the internal carotid artery (▶Fig. 6.7).

Any vascular disease involving the arteries between the heart and the ophthalmic artery may result in ocular ischemia and visual loss.
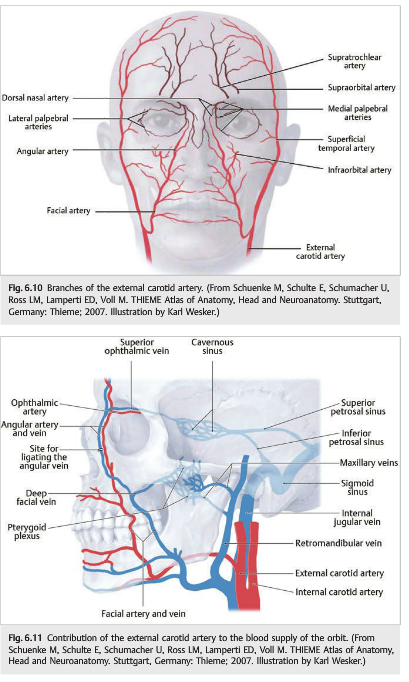
The external carotid artery and its branches also contribute to the vascularization of the eye and orbital contents. In cases of internal carotid artery stenosis or occlusion, the entire ocular vascularization may originate from the external carotid artery. In this situation, there may be a steal phenomenon from the eye to the brain, and the flow may be reversed in the ophthalmic artery so that most of the blood flow contributes to the vascularization of the ipsilateral cerebral hemisphere.
Branches of the ophthalmic artery (▶Fig. 6.8 and ▶Fig. 6.9) include the central retinal artery to the inner retina; the short posterior ciliary arteries to the choroid and optic nerve; the long posterior ciliary arteries to the ciliary body and iris; and the anterior ciliary arteries, which arise from the vessels of the rectus muscles. Occlusion of the ophthalmic artery results in complete ocular ischemia, whereas occlusion of the central retinal artery results in retinal ischemia.

Pearls
The external carotid artery is important for collateral circulation for the orbit and for the brain when there is severe occlusive disease of the internal carotid artery (▶Fig. 6.10, and ▶Fig. 6.11).
Mechanisms of Vascular TMVL
The mechanisms of vascular TMVL are emboli, hypoperfusion of the eye (hemodynamic TMVL), vasculitis (usually giant cell arteritis), arterial vasospasm (central retinal artery), and venous congestion (central retinal vein).
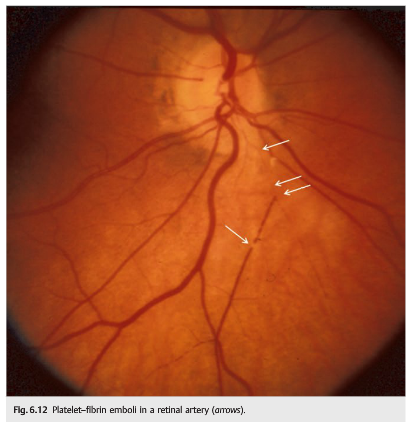
● Emboli into the retinal circulation (▶Fig. 6.12, ▶Fig. 6.13, and ▶Fig. 6.14) (central and branch retinal arteries) most often result from lesions of the common or internal carotid arteries that embolize material to the retinal circulation. With emboli, most commonly a black or dark shade spreads across the visual field of the affected eye, disappearing after a few minutes. Occasionally, emboli may be observed ophthalmoscopically as they pass through the retinal arterioles.

Pearls
Emboli (in the central retinal artery or the ophthalmic artery) represent the most common cause of transient or permanent retinal ischemia, which should warrant an immediate workup looking for a source of emboli. Carotid disease is the most common cause of retinal ischemia.
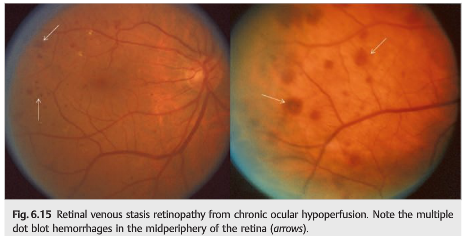
● Hypoperfusion of the eye (▶Fig. 6.15 and ▶Fig. 6.16) is seen in severe stenosis of the carotid circulation, which causes TMVL due to retinal or choroidal hypoperfusion. Ocular hypoperfusion may be associated with transient but prolonged visual loss(several minutes to hours) and positive visual phenomena. TMVL is classically induced by situations that either decrease perfusion pressure (e.g., postural change) or increase retinal oxygen demand (e.g., exposure to bright light), or when blood flow is shunted elsewhere systemically (e.g., after eating a meal or during exercise). Venous stasis retinopathy or ischemic ocular syndrome with development of ocular neovascularization may be observed. Revascularization procedures restoring normal ocular perfusion may prevent the development of ocular ischemic syndrome.

● Giant cell arteritis is an important cause of recurrent TMVL in subjects older than age 50. The ocular examination may be normal or may show optic nerve edema, suggesting impending permanent visual loss from arteritic anterior ischemic optic neuropathy. These patients need to be treated with high-dose steroids emergently to prevent permanent visual loss (see Chapter 20).
● Vasospasm of the central retinal artery may produce episodes of isolated, painless, sudden, complete loss of vision in one eye, usually lasting between 30 seconds and 1 minute. Vasospasm most often affects young, healthy people, and its cause is unclear. The prognosis is excellent without subsequent risk of ocular or cerebral infarction. Antiplatelet agents or calcium channel inhibitors are usually prescribed.
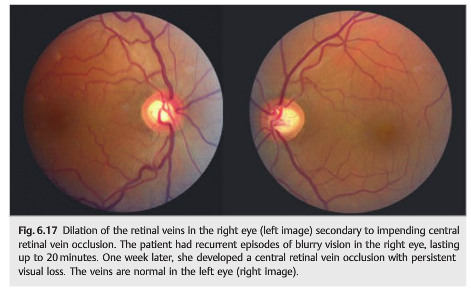
● Central retinal vein occlusion (▶Fig. 6.17) may be preceded by episodes of transient monocular blurry vision. These episodes last longer than with arterial ischemia, and the visual loss is usually incomplete.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.