Questions:
1. What is the preferred term for abrupt and temporary vision loss in one eye?
2. What is the most common cause of transient monocular vision loss?
3. What is amaurosis fugax?
4. What is the first step in evaluating transient vision loss?
5. Why is it important to determine whether transient vision loss is unilateral or bilateral?
6. What 3 items are included in the differential diagnosis of transient binocular visual loss?
7. What are the characteristics of an occipital seizure?
8. Are occipital seizures more common in children or adults?
9. What are the characteristics of an occipital transient ischemic attack?
________________________________________
Questions with answers:
1. What is the preferred term for abrupt and temporary vision loss in one eye?
Transient monocular visual loss (TMVL)
2. What is the most common cause of transient monocular vision loss?
Transient ocular ischemia
3. What is amaurosis fugax?
Temporary partial or complete loss of sight in one or both eyes that is caused by an abrupt reduction in blood flow (ischemia) to an eye.
4. What is the first step in evaluating transient vision loss?
Determine whether the transient vision loss is unilateral or bilateral.
5. Why is it important to determine whether transient vision loss is unilateral or bilateral?
A unilateral transient loss of vision localizes the lesion to the optic nerve or the eye.
6. What 3 items are included in the differential diagnosis of transient binocular visual loss?
1. Migrainous Visual Aura
2. Occipital Transient Ischemic Attack
3. Occipital Seizure
7. What are the characteristics of an occipital seizure?
The patient typically complains of recurrent, brief, simple, positive visual phenomena, such as flashes of light or bubbles. They are binocular and they may be localized to a hemifield or diffuse within the entire field of vision.
8. Are occipital seizures more common in children or adults?
Children
9. What are the characteristics of an occipital transient ischemic attack?
1. Occurs in older patients.
2. Unilateral occipital TIA from the posterior cerebral artery manifests as a transient homonymous hemianopia.
3. Occipital TIAs are typically sudden in onset and last only a few minutes.
4. Complete binocular visual loss may represent a TIA in the distribution of the basilar artery.
5. Vertebrobasilar ischemia may have associated symptoms: vertigo, dizziness, imbalance, diplopia, bilateral extremity weakness.
6. There may be associated headache, especially over the brow contralateral to the visual field loss, but the pain is usually coincident with the visual loss, rather than following the visual loss as in migraine.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
6 Transient Visual Loss
It is sometimes difficult to decide whether an episode of transient visual loss occurred in one eye (monocular) or both (binocular). Very few patients realize that binocular hemifield (homonymous) visual field loss affects the fields of both eyes. They will usually localize it to the eye that lost its temporal field. The best clues to the fact that transient visual loss was actually binocular are reading impairment (monocular visual loss does not impair reading unless the unaffected eye had prior vision impairment)and visual loss confined to a lateral hemifield, that is, to the right or left of midline with respect to the vertical meridian (monocular visual loss does not usually cause that pattern of visual loss).
This chapter complements the overview of visual loss given in Chapter 5 and provides differential diagnoses and suggested management for transient monocular and binocular visual loss.
Pearls
The most important step in evaluating a patient with transient visual loss is to establish whether or not the visual loss is monocular (lesions of the eye or anterior visual pathways) or binocular (lesions of the chiasm or retrochiasmal visual pathways).
6.1 Transient Binocular Visual Loss
6.1.1 Differential Diagnosis
Migrainous Visual Aura
Visual aura associated with migraine is the most common cause of transient binocular visual loss (▶Fig. 6.1). The patient typically notes a small scotoma in homonymous portions of the visual field, surrounded by jagged, luminous, shimmering edges. The scotoma enlarges over several minutes, then gradually disappears. The visual loss may enlarge to a complete homonymous hemianopia. A hemicranial throbbing headache characteristically follows (see Chapter 19).

Some patients experience the visual aura of migraine without associated headache. The vision and visual fields return to normal after the aura, usually within 20 to 30 minutes (always less than 1 hour).
Pearls
Although migrainous visual aura is binocular by definition (since it originates from the occipital lobe), many patients do not recognize the visual phenomena as being in both eyes, especially when they involve only one hemifield. The relatively long duration of visual phenomena, the progressive buildup of symptoms (“migrainous march”), and the richness of visual phenomena strongly suggest migrainous visual auras, even when the patient thinks the visual symptoms were only in one eye.
Occipital Transient Ischemic Attack
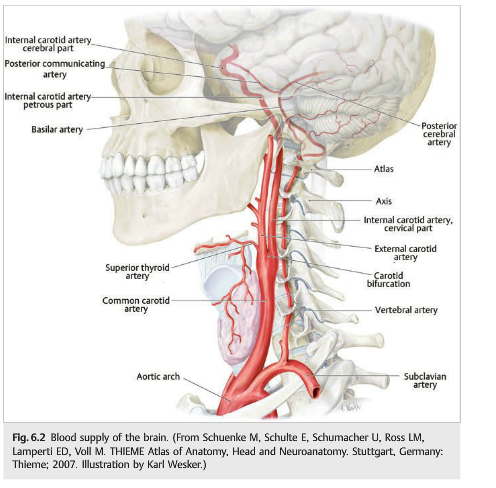
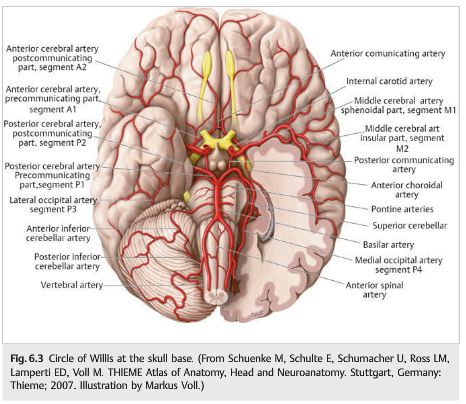
In older patients, episodes of transient, complete binocular visual loss may represent transient ischemic attack (TIA) in the distribution of the basilar artery or of the posterior cerebral arteries. A unilateral occipital TIA manifests as a transient homonymous hemianopia. As opposed to migraine, hemianopic events of ischemic origin are typically sudden in onset and last only a few minutes. There may be associated headache, especially over the brow contralateral to the visual field loss, but the pain is usually coincident with the visual loss, rather than following the visual loss as in migraine. TIAs in the anterior circulation produce ipsilateral monocular visual loss, whereas TIAs in the posterior circulation produce binocular visual loss (often contralateral homonymous hemianopia). This is explained by the anatomy of the blood supply to the brain (▶Fig. 6.2 and ▶Fig. 6.3). The internal carotid arteries provide the blood supply to the anterior part of both cerebral hemispheres and to the eyes. The vertebrobasilar system provides the blood supply to the posterior part of both cerebral hemispheres (including the occipital lobes)and to the posterior fossa (brainstem and cerebellum) (▶Fig. 6.2). The occipital lobes are vascularized by the posterior cerebral arteries, which originate from the basilar artery (▶Fig. 6.3). Basilar artery stenosis or occlusion may result in bilateral occipital ischemia and bilateral complete visual loss (cerebral blindness). Posterior cerebral artery occlusion usually produces unilateral occipital ischemia with contralateral homonymous hemianopia.
Occipital Seizure
Occipital seizures can occur at any age but are more common in children. They may be primary or secondary to an occipital lesion. The patient typically complains of recurrent and brief, simple, positive visual phenomena, such as flashes of light or bubbles. They are binocular and they may be localized to a hemifield or diffuse within the entire field of vision. ▶Table 6.1 compares the characteristics of migrainous visual aura, occipital TIA, and occipital seizure. Other less common causes of transient binocular visual loss are head trauma, especially in children; hypertensive encephalopathy; toxemia of pregnancy; and toxicity of drugs, such as cyclosporine, which may result in cerebral blindness lasting hours or days (see ▶Fig. 5.25).

6.2 Transient Monocular Visual Loss
Transient monocular visual loss (TMVL) is the preferred term for abrupt and temporary visual loss in one eye. TMVL most often results from transient ocular ischemia (so-called amaurosis fugax), but it may also result from other mechanisms such as disc edema and numerous ocular diseases. See the discussion in Chapter 5.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.