Questions:
10. Other than vascular disease, what 10 conditions can cause transient monocular visual loss?
11. What is Uhthoff’s phenomenon?
12. What conditions should be considered in the absence of an RAPD in cases where the cause of unilateral or asymmetric visual loss is not apparent?
13. What simple clinical test may help in determining if a maculopathy is present where the cause of unilateral or asymmetric visual loss is not apparent?
14. What are five retinal conditions that may mimic optic neuropathies?
15. What is the acquired idiopathic blind spot enlargement syndrome (AIBSE)?
16. What are 4 bilateral retinal conditions that may be difficult to distinguish from bilateral symmetric primary optic neuropathies?
17. What is the fundus appearance early in the course of cone dystrophies?
18. What specific historical items should be sought in cases of unexplained monocular visual acuity loss but with a normal visual field?
19. What exam findings may be found that help confirm the diagnosis of amblyopia?
20. Why should the blood pressure be checked in patients with a history of transient vision loss?
21. What are the findings of the posterior reversible encephalopathy syndrome?
____________________________________
Questions with answers:
10. Other than vascular disease, what 10 conditions can cause transient monocular visual loss?
1. dry eyes
2. keratoconus
3. hyphema
4. angle closure glaucoma
5. retinal detachment
6. papilledema
7. optic disk drusen
8. congenitally anomalous optic discs
9. gaze-evoked optic nerve compression
10. Uhthoff’s phenomenon.
11. What is Uhthoff’s phenomenon?
The worsening of vision with increased body temperature (e.g. exercise, hot tubs). It occurs in MS.
12. What conditions should be considered in the absence of a RAPD in cases where the cause of unilateral or asymmetric visual loss is not apparent?
Maculopathies and for unilateral visual loss also consider amblyopia.
13. What simple clinical test may help in determining if a maculopathy is present where the cause of unilateral or asymmetric visual loss is not apparent?
The photostress test: maculopathies have a prolonged recovery time, optic neuropathies have a normal recovery time.
14. What are five retinal conditions that may mimic optic neuropathies?
1. central serous retinopathy
2. macular degeneration
3. macular hole
4. cystoid macular edema
5. acquired idiopathic blind spot enlargement syndrome.
15. What is the acquired idiopathic blind spot enlargement syndrome (AIBSE)?
AIBSE is characterized by sudden onset of enlargement of the physiologic blind spot. The patient is aware of a monocular scotoma temporally with photopsias in the scotomatous field. It affects mostly women between the ages of 20 and 40 years. Visual acuity and color vision are typically spared, and an RAPD is present in > 50%. Ophthalmoscopy and fluorescein angiography are often normal. However, subtle grayish discoloration of the peripapillary retina is seen. Electroretinogram is often abnormal. AIBSE generally resolves over several weeks or months but occasionally will recur in the same or opposite eye.
16. What are 4 bilateral retinal conditions that may be difficult to distinguish from bilateral symmetric primary optic neuropathies?
1. Vitamin A deficiency retinopathy
2. Toxic retinopathies (e.g. plaquenil)
3. Carcinoma/melanoma-associated paraneoplastic retinopathies
4. Retinal dystrophies (especially cone dystrophies).
17. What is the fundus appearance early in the course of cone dystrophies?
Often there is a relatively normal-appearing fundus examination except for bilateral temporal disk pallor, and retinal arterial attenuation. Changes in the appearance of the macula, often resembling a bulls-eye, can be delayed.
18. What specific historical items should be sought in cases of unexplained monocular visual acuity loss but with a normal visual field?
Ask about a history of:
1. uncorrected refractive error
2. “lazy eye”
3. strabismus surgery
4. patching during childhood
5. other “vision therapy”
Amblyopia usual has a normal visual field or mild generalized depression and may have a minimal RAPD.
19. What exam findings may be found that help confirm the diagnosis of amblyopia?
1. Improvement of visual acuity with testing of isolated letters (crowding phenomenon).
2. No or a small RAPD (0.3–0.6 log unit at most)
20. Why should the blood pressure be checked in patients with a history of transient vision loss?
Reversible posterior leukoencephalopathy most often results from malignant systemic hypertension, eclampsia, or central nervous system toxicity from immunosuppressive drugs (e.g. cyclosporine or tacrolimus).
21. What are the findings of the posterior reversible encephalopathy syndrome?
Posterior reversible encephalopathy syndrome is characterized by headache, altered mental status, seizures, and visual disturbances (transient visual loss, scotomata, photopsias, dimming of vision). MRI shows edema involving the white matter of the cerebral posterior regions, especially parieto-occipital lobes, but frontal and temporal lobes may be involved. The abnormalities visible on neuroimaging are reversible, and the visual prognosis is usually excellent.
____________________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
5.2 Monocular Visual Loss
Monocular visual loss always results from lesions anterior to the chiasm (the eye or the optic nerve). Transient or permanent monocular visual loss may result from various mechanisms. Those resulting from disorders of the eye itself are usually easily diagnosed by the ophthalmologist. Optic neuropathies and some retinal and ocular vascular disorders that cause monocular visual loss may present to the neurologist.
Any lesion involving the eye (▶Fig. 5.2) or optic nerve may produce monocular visual loss, including the following:
● Refractive errors
● Corneal diseases
● Anterior chamber inflammation (anterior uveitis)
● Anterior chamber hemorrhage (hyphema)
● Lens opacities (cataract), dislocation
● Vitreous hemorrhage
● Vitreous inflammation (posterior uveitis)
● Retinal diseases
● Choroidal diseases
● Optic neuropathies

5.2.1 Causes of Transient Monocular Visual Loss
Numerous ocular disorders as well as transient ocular ischemia may produce episodes of transient monocular visual loss (TMVL) (see Chapter 6).
There are three main causes of TMVL: vascular disorders, ocular diseases, and optic nerve disorders:
● The most common vascular disorder of the eye is sometimes referred to as amaurosis fugax, the temporary loss of vision of one eye caused by decreased blood flow (ischemia) to the retina.
● Orbital (ophthalmic artery), retinal (central retinal artery and its branches), optic nerve (short posterior ciliary arteries), and choroidal (posterior ciliary arteries) ischemia can all produce TMVL.
● Ocular diseases involving the anterior segment of the eye that can cause TMVL include dry eyes, keratoconus, hyphema, and angle closure glaucoma. Retinal detachment can also rarely produce transient visual loss.
● Optic nerve disorders that can cause TMVL include papilledema, optic disc drusen, and congenitally anomalous optic discs, all of which can produce transient visual obscurations. Gaze-evoked transient monocular visual loss can be the result of optic nerve compression. The Uhthoff phenomenon occurs in patients with optic neuropathies, (especially of demyelinating etiology), whose vision may worsen with heat or exercise.
5.2.2 Ocular Causes of Permanent Monocular Visual Loss
In cases of permanent visual loss, the ocular examination usually allows direct visualization of the cause of visual loss. It is when the eye itself appears normal, or when the optic nerve is not normal, that a neuro-ophthalmic disorder is suspected.
Permanent visual loss may result from disorders involving the anterior segment of the eye (seen with a penlight or direct ophthalmoscope at bedside, or with a slit lamp)or from disorders involving the posterior segment of the eye (seen with a direct ophthalmoscope, with a slit lamp, or with an indirect ophthalmoscope).
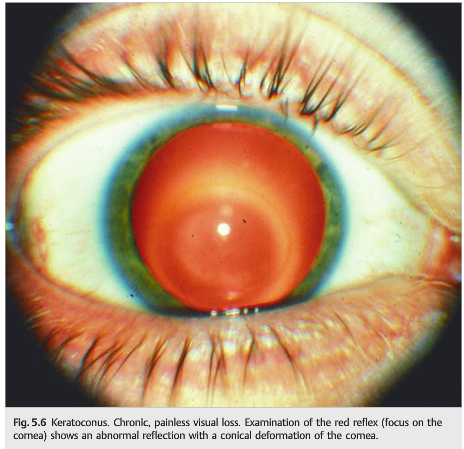
▶Fig. 5.3, ▶Fig. 5.4, ▶Fig. 5.5, ▶Fig. 5.6, ▶Fig. 5.7, and ▶Fig. 5.8 show examples of anterior segment disorders presenting with acute or chronic visual loss.





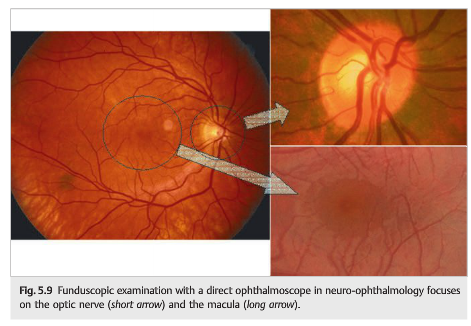
Funduscopic examination is essential in patients with visual loss (see Chapter 2). Optic neuropathies and retinal disorders involving the macula are common causes of central visual loss in patients with clear ocular media. Neurologists need to be able to reliably examine the optic nerve and the macula, which can be done with a direct ophthalmoscope at the bedside (▶Fig. 5.9).
Ophthalmologists use the slit lamp and lenses of various powers to visualize the optic nerve and macula (posterior pole) and an indirect ophthalmoscope to examine the entire retina and its vasculature. The slit lamp and the indirect ophthalmoscope require more practice than the direct ophthalmoscope and are only rarely used by neurologists. These techniques allow stereo views of the fundus and therefore better appreciation of optic nerve elevation, cupping, and contour, as well as macular thickness and edema.
The red reflex is the first step of the funduscopic examination (▶Fig. 5.10; see Chapter 2) and is used to screen for opacities or irregularities in the cornea, lens, or vitreous.

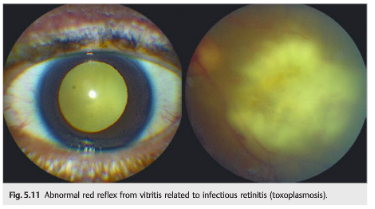
An abnormal red reflex suggests a problem with the ocular media or severe retinal disease involving the posterior pole (▶Fig. 5.11). Patients with optic neuropathies have a normal red reflex.
When the red reflex is abnormal and the fundus cannot be visualized (hazy or no view), then a media opacity is obstructing the view (▶Fig. 5.12a), and B-scan ultrasonography of the eye is helpful in this setting as it may provide an explanation for the media opacity and allow examination of the retina to see if it is attached or not and if there is a retinal tear (▶Fig. 5.12b) (see Chapter 4).

Pearls
● Use the red reflex (with the ophthalmoscope) to look for media opacities or to screen for visual abnormalities in young children.
● A normal red reflex indicates transparent ocular media
● An asymmetric red reflex indicates a problem with the ocular media, a retinal disorder, high refractive error, or ocular misalignment (strabismus). Checking for asymmetry of the red reflex is therefore a good way to screen young children for ocular disorders and amblyopia.
● A white reflex (also called leukocoria) suggests that something “white” is in the way. Retinoblastoma, congenital cataract, and retrolental fibroplasia are the most important causes of leukocoria in children.
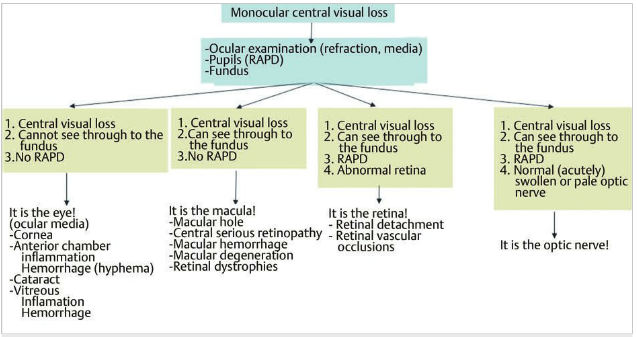
▶Fig. 5.13 provides an anatomical approach to the patient with monocular visual loss
Fig.5.13 The anatomical localization of monocular visual loss.
5.2.3 Retinal Masqueraders of Optic Neuropathies
Retinal disorders involving the inner retinal layers (i.e., near the vitreous), such as central retinal artery occlusion, are usually easily identified on funduscopic examination (see Chapter 7).
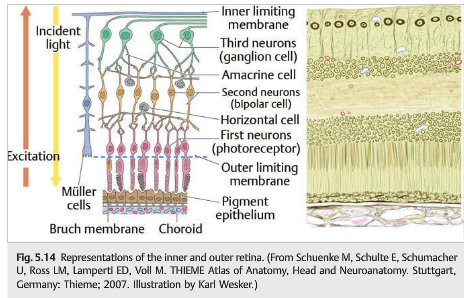
When the outer retina (deeper layers of the retina, including the photoreceptors and the underlying retinal pigment epithelium; ▶Fig. 5.14) is affected, the fundus is often normal initially.
Some retinal disorders, especially those involving the macula and the outer layers of the retina, can mimic a unilateral or bilateral optic neuropathy. The absence of a RAPD should lead the examiner to suspect a problem removed from the optic nerve in cases of unilateral or asymmetric visual loss (▶Table 5.1).

In general, maculopathies produce visible fundus abnormalities that allow a correct diagnosis. However, they may be missed, subtle, or absent. Fluorescein angiography, optical coherence tomography (OCT), and electroretinogram (especially multifocal electroretinogram) can be very helpful in this setting (see Chapter 4).
Examples of retinal disorders that may mimic optic neuropathies are central serous retinopathy, macular degeneration, macular hole, cystoid macular edema, and acquired enlargement of the physiologic blind spot.
Central serous retinopathy is common, particularly in young men (▶Fig. 5.15). In this condition, fluid accumulates in the macular subretinal space and produces central visual loss. Visual loss is acute, painless, and associated with metamorphopsia and a central scotoma. OCT (▶Fig. 5.15c) and fluorescein angiography have a characteristic appearance and will confirm the diagnosis.

Macular degeneration is common in elderly patients. It is bilateral, progressive, and associated with macular drusen (yellow-white deposits with irregular borders—different from the drusen found in optic nerves) and retinal pigment epithelium (RPE) changes (hypo- or hyperpigmentation) (dry age-related macular degeneration)(▶Fig. 5.16).

Progressive deterioration of the deeper retinal layers and RPE may result in serous retinal detachment, RPE detachment, or subretinal neovascularization with hemorrhage and fibrosis (wet age-related macular degeneration), which are best identified with OCT and fluorescein angiography.
A macular hole is a hole in the center of the macula overlying the foveola and responsible for central visual loss (▶Fig. 5.17). It is secondary to vitreoretinal traction and occurs most often in elderly patients or after ocular trauma.

Cystoid macular edema (CME) occurs mostly in ocular inflammation and after cataract surgery (▶Fig. 5.18a). It results from perifoveal capillary leakage. There is thickening of the macular region by edema. OCT and fluorescein angiography are often obtained to confirm CME (▶Fig. 5.18b).

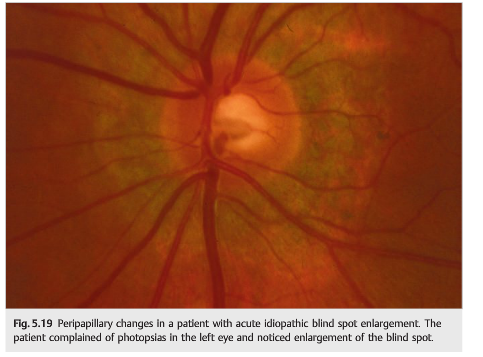
Acquired enlargement of the physiologic blind spot, both symptomatic and asymptomatic, is usually the result of swelling of the optic nerve head. Occasionally, however, blind spot enlargement may occur with a normal-appearing optic nerve in the setting of outer retinal dysfunction, the so-called acute idiopathic blind spot enlargement (AIBSE) syndrome (part of the group of disorders included in acute zonal occult outer retinopathy [AZOOR]). AIBSE (▶Fig. 5.19) is characterized by sudden onset of enlargement of the physiologic blind spot (the patient is aware of a monocular scotoma temporally) and photopsias in the scotomatous field. It affects mostly women between the ages of 20 and 40 years. Visual acuity and color vision are typically spared, and there may or may not be a RAPD (present<50% of the time). Ophthalmoscopy and fluorescein angiography are often normal. However, subtle grayish discoloration of the peripapillary retina (around the disc) may be seen over time. The electroretinogram is often abnormal. AIBSE generally resolves over several weeks or months but occasionally will recur in the same or opposite eye.
5.2.4 Amblyopia
In cases of unexplained monocular visual loss, previously unrecognized amblyopia must be considered.
Amblyopia is defined as reduction of best corrected central visual acuity in the absence of a visible organic lesion corresponding to the degree of visual loss. It will have been present since early childhood and represents the normal brain “not listening” as well to one of the two different afferent inputs.
Causes of amblyopia include the following:
● Uncorrected anisometropia (a difference in refractive error between the two eyes)
● Uncorrected astigmatism
● Strabismus (misalignment of the two eyes, resulting in suppression of one eye’s vision)
● Ocular occlusion (e.g., from congenital ptosis)
Consider amblyopia in a patient with unexplained monocular visual loss with normal ocular appearance and a history of uncorrected refractive error, “lazy eye,” strabismus surgery, or patching during childhood; improvement of visual acuity with testing of isolated letters (crowding phenomenon); no or small RAPD (0.3–0.6 log unit at most); and a normal visual field (or mild generalized depression).
5.3 Binocular Visual Loss
Binocular visual loss results from lesions of both eyes, of both optic nerves, or of the chiasm or retrochiasmal visual pathways (▶Fig. 5.20; see also Chapter 3).

Acute lesions involving both eyes, or both optic nerves, simultaneously are very rare. Any lesion involving the chiasm or the intracranial visual pathways will produce binocular visual loss or visual field defects, including lesions of the optic tract, lateral geniculate body, optic radiations, and occipital lobe.
Pearl
Lesions involving one side of the intracranial visual pathways produce a contralateral homonymous hemianopia, but the visual acuity is not affected. Lesions involving both occipital lobes may be responsible for severely decreased visual acuity in both eyes; the amount of visual acuity loss is symmetric in both eyes unless there is a superimposed ocular reason for decreased visual acuity.
5.3.1 Bilateral Retinopathies Relevant to Neuro-ophthalmologists
Bilateral retinal disorders may be difficult to distinguish from bilateral symmetric primary optic neuropathies because a RAPD will also be absent. There is a group of retinal disorders, commonly designated retinal degenerations or dystrophies, in which secondary optic disc pallor occurs bilaterally. Arterial attenuation is common in these retinal disorders. Macular changes may be delayed, and the diagnosis maybe difficult without electroretinography. Fundus autofluorescence photography of the macula is often helpful to demonstrate early macular changes (see ▶Fig. 4.5; ▶Fig. 5.21).


These retinopathies include the following:
● Vitamin A deficiency retinopathy
● Toxic retinopathies (e.g., hydroxychloroquine) (see ▶Fig. 5.21)
● Carcinoma- and melanoma-associated paraneoplastic retinopathies
● Retinal dystrophies (especially cone dystrophies)
Cone dystrophies are characterized by bilateral loss of central vision (visual acuities typically slowly deteriorate to the 20/200 to 20/400 level) (▶Fig. 5.22 and ▶Fig. 5.23), profound color vision deficits, photophobia, and an inability to see as well in bright as in dim light (hemeralopia), a relatively normal-appearing fundus examination except for bilateral temporal disc pallor, and retinal arterial attenuation. Changes in the appearance of the macula, often resembling a bull’s-eye, can be delayed. Cone dystrophies are usually sporadic, although inherited forms have been reported.


Electroretinogram is diagnostic in these disorders. When anomalies are limited to the macula, a full-field electroretinogram may be normal, whereas a multifocal electroretinogram is diagnostic.
Paraneoplastic retinopathies (cancer-associated retinopathy [CAR] and melanoma- associated retinopathy [MAR]) follow a more rapid course than the other degenerative retinopathies (▶Fig. 5.24). CAR may cause early central or paracentral loss of vision. However, initial presentation is often that of bilateral visual loss with minimal or no funduscopic findings. The electroretinogram confirms the retinopathy. Serum antibodies (CAR antibodies) and discovery of a primary neoplasm confirm the diagnosis.

5.3.2 Causes of Transient or Permanent Binocular Visual Loss
Causes of transient or permanent binocular visual loss from retrochiasmal lesions are as follows:
● Vascular
○ Vertebrobasilar ischemia (posterior cerebral artery territory)
○ Cerebral anoxia
○ Cerebral venous thrombosis (superior sagittal sinus
○ Hypertensive encephalopathy
○ Malignant systemic hypertension (▶Fig. 5.25)
○ Eclampsia
● Head trauma
● Occipital mass (e.g., tumor, abscess, or hemorrhage)
● Demyelinating disease
● Infection
○ Occipital abscess
○ Meningitis
○ Progressive multifocal leukoencephalopathy
○ Creutzfeldt–Jakob disease
● Central nervous system toxicity
○ Cyclosporine
○ Tacrolimus (FK-506)
○ Mercury
● Metabolic
○ Hypoglycemia
○ Porphyria
○ Hepatic encephalopathy
● Migraine (visual aura)
● Occipital lobe seizures
● Degenerative
○ Alzheimer disease
○ Posterior cortical atrophy
Reversible posterior leukoencephalopathy most often results from malignant systemic hypertension, eclampsia, or central nervous system toxicity from cyclosporine or tacrolimus.

Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Thieme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.