Questions:
Acquired Nystagmus
9. What are the characteristics, concerns, lesion location, and treatment for gaze-evoked nystagmus?
10. What are the characteristics, concerns, lesion location, and treatment for nystagmus with positional vertigo?
11. What are the characteristics, concerns, lesion location, and treatment for downbeat nystagmus?
12. What are the characteristics, concerns, lesion location, and treatment for upbeat nystagmus?
13. What are the characteristics, concerns, lesion location, and treatment for periodic alternating nystagmus?
14. What are the characteristics, concerns, and lesion location for rebound nystagmus?
15. What are the characteristics and lesion location Brun nystagmus?
16. What are the characteristics, concerns, and treatment for dissociated jerk nystagmus?
17. What are the characteristics, concerns, lesion location, and treatment for acquired pendular nystagmus?
18. What are the characteristics, concerns, lesion location, and treatment for seesaw nystagmus?
19. What are the characteristics, lesion location, and treatment for oculopalatal myoclonus?
20. What are the characteristics, concerns, lesion location, and treatment for oculomasticatory myorhythmia?
21. What are the characteristics, concerns, and treatment for Wernicke encephalopathy?
22. Which patterns of jerk nystagmus have localizing/diagnostic value?
23. Which patterns of pendular nystagmus have localizing/diagnostic value?
__________________________________________________
Questions with answers:
9. What are the characteristics, concerns, lesion location, and treatment for gaze-evoked nystagmus?Characteristics
Gaze-evoked is the most common type of nystagmus.
Absent in the primary position.
Not visually disabling.
Jerk nystagmus beats in the direction of gaze.
Concerns It results from impairment in eccentric gaze-holding mechanisms, such as from sedative medications/anticonvulsants and brainstem and cerebellar lesions (central vestibular dysfunction).
Location Brainstem and cerebellar lesions
Treatment None, it is not visually disabling.
10. What are the characteristics, concerns, lesion location, and treatment for nystagmus with positional vertigo?Characteristic
Positional nystagmus occurs when head is in a specific position.
When the Dix–Hallpike maneuver is performed, nystagmus is seen.
Concerns Most patients have benign paroxysmal positional vertigo (BPPV) from a peripheral lesion, usually canalolithiasis or cupulolithiasis in the posterior semicircular canal.
Positional vertigo may also occur with central nervous system disease.
Location Usually canalolithiasis or cupulolithiasis in the posterior semicircular canal.
Treatment BPPV does not respond well to medications but may have a long-term favorable response to numerous maneuvers aimed at dislodging the debris from the posterior semicircular canal.
Acquired Central Nystagmus
11. What are the characteristics, concerns, lesion location, and treatment for downbeat nystagmus?
Characteristics
It is an acquired central nystagmus.
It is a type of jerk nystagmus, with fast phase downward in primary position.
The nystagmus decreases in upgaze and worsens in downgaze; it is usually most prominent in lateral and down gaze.
Oscillopsia is usually prominent because the nystagmus is present in primary position and in downgaze, the preferred reading position.
Concerns It is commonly seen in cerebellar degenerations; paraneoplastic syndromes; Chiari malformation; encephalitis; trauma; hypomagnesemia; thiamine deficiency; B12 deficiency; and toxicity with lithium, alcohol, amiodarone, toluene, phenytoin, and carbamazepine.
It is often idiopathic.
Location Downbeat nystagmus is caused by lesions at the cervicomedullary junction, foramen magnum, vestibulocerebellum, and medulla.
Treatment
1. Clonazepam, baclofen, gabapentin, memantine, and 3,4-diaminopyridine are commonly (off-label) used, but they are frequently only partially successful or unsuccessful.
2. Patients should be advised to avoid looking down and to not use glasses with bifocal or progressive lenses.
3. As downbeat nystagmus is generally less pronounced in upward gaze, base-down prisms sometimes help to reduce oscillopsia during reading in some patients.
4. A trial of base-out prisms (to induce convergence) may dampen down-beat nystagmus.
12. What are the characteristics, concerns, lesion location and treatment for upbeat nystagmus?
Characteristics It is an acquired central nystagmus. Upbeat nystagmus is a type of jerk nystagmus with fast phase upward in primary position. It often worsens in upgaze.
Concerns It is commonly seen in Wernicke encephalopathy and encephalitis.
Location Medulla, cerebellar vermis, and midbrain.
Treatment
1. Aminopyridines and baclofen may dampen upbeat nystagmus.
2. Patients should avoid looking up and not use glasses with progressive lenses.
3. Base-up prisms in reading glasses can be used to force the eyes downward.
13. What are the characteristics, concerns, lesion location and treatment for periodic alternating nystagmus
Characteristics
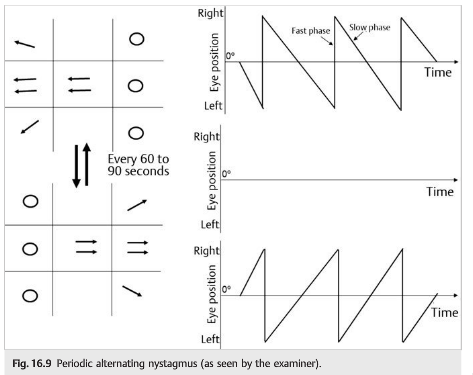
It is an acquired central nystagmus. Periodic alternating nystagmus is a type of horizontal jerk nystagmus that alternates direction in primary position (i.e., jerk nystagmus to the right for about 60 to 90 seconds, which diminishes, only to begin beating to the left for another 60 to 90 seconds).
Patients may have a periodic alternating head turn to minimize the nystagmus, and oscillopsia is usually present.
Concerns It is commonly seen in multiple sclerosis, cerebellar degenerations, Chiari malformations, trauma, hepatic encephalopathy, and albinism, as well as with use of anticonvulsants and lithium.
Location Cerebellum, particularly the nodulus and uvula, and by lesions of the cervicomedullary junction.
Treatment Baclofen
14. What are the characteristics, concerns, and lesion location for rebound nystagmus?
Characteristics
It is an acquired central nystagmus.
Rebound nystagmus is characterized by gaze-evoked nystagmus that wanes and then reverses direction.
Concerns Rebound nystagmus is seen in some patients with gaze-evoked nystagmus.
Location Cerebellar disorders and lesions of the medulla (in the region of the nucleus prepositus hypoglossi and medial vestibular nucleus).
15. What are the characteristics and lesion location Brun nystagmus?
Characteristics
It is an acquired central nystagmus.
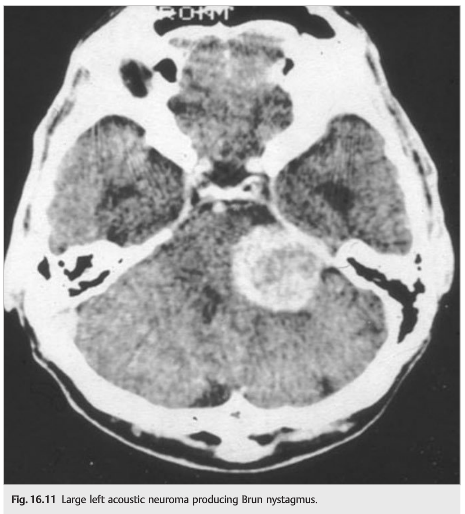
It is a combination of a unilateral peripheral vestibular nystagmus from 8th CN tumor and a gaze-paretic central nystagmus as the tumor compresses the pons.
The nystagmus is characterized by a high-frequency, low-amplitude nystagmus on looking away from the lesion, beating in the direction of gaze (due to the vestibular lesion), and a low-frequency, high-amplitude horizontal nystagmus on looking toward the lesion, beating in the direction of gaze (due to defective gaze holding).
Location Is caused by large tumors of the cerebellopontine angle.
16. What are the characteristics, concerns, and treatment for dissociated jerk nystagmus?
Characteristics
It is an acquired central nystagmus.
One of the most common types of nystagmus is acquired pendular nystagmus, which is visually disabling because of severe oscillopsia.
Concerns Multiple sclerosis is the most common cause.
Treatment Oscillopsia may improve with gabapentin, memantine, clonazepam, or valproate.
17. What are the characteristics, concerns, lesion location, and treatment for acquired pendular nystagmus?
Characteristics
It is an acquired central nystagmus.
One of the most common types of nystagmus is acquired pendular nystagmus, which is visually disabling because of severe oscillopsia.
Acquired pendular nystagmus may be horizontal, vertical, or a combination (circular, elliptical, or windmill pendular nystagmus).
It may be symmetric, dissociated, or frankly monocular.
Concerns Multiple sclerosis is the most common cause.
Other common etiologies include brainstem demyelination, stroke, hemorrhage, or tumor.
Less common causes include Pelizaeus Merzbacher disease, mitochondrial cytopathy, Cockayne syndrome, adrenoleukodystrophy, and toxins (eg, toluene).
Location Imaging studies have revealed lesions in the pontine tegmentum and cerebellar nodulus.
Treatment Oscillopsia may improve with gabapentin, memantine, clonazepam, or valproate.
18. What are the characteristics, concerns, lesion location, and treatment for seesaw nystagmus?
Characteristics
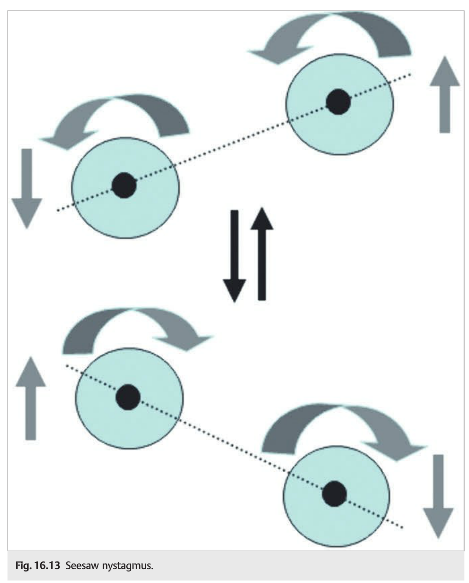
Seesaw nystagmus is defined as pendular nystagmus with elevation and intorsion of one eye simultaneous with depression and extorsion of the other eye, followed by a reversal of the cycle, so that the eyes move like a seesaw
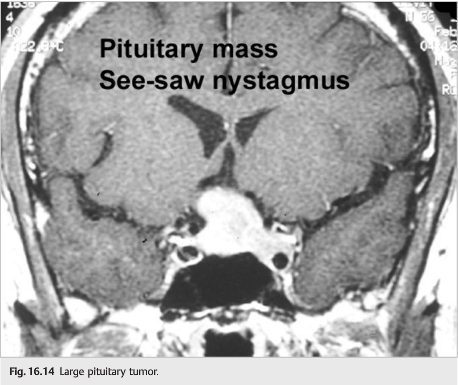
Concerns Parasellar, suprasellar, or third ventricular mass, Brainstem and thalamic stroke, Multiple sclerosis, Trauma (chiasmal disruption), Arnold-Chiari malformation. Hydrocephalus, Syringobulbia, Paraneoplastic encephalitis (with testicular cancer and anti-Ta antibodies), Septo-optic dysplasia, retinitis pigmentosa, and cone degeneration, and Congenital seesaw nystagmus.
Location It is most often caused by parasellar lesions and may be seen with pituitary tumors, craniopharyngiomas, septo-optic dysplasia, and brainstem lesions (especially in the midbrain).
Treatment Alcohol, Clonazepam, and Memantine
19. What are the characteristics lesion location and treatment for oculopalatal myoclonus?
Characteristics
Oculopalatal myoclonus is a type of vertical pendular nystagmus coexisting with a tremor of the palate and/or facial muscles, larynx, and diaphragm.
It is present during sleep. It usually develops months after an infarction, hemorrhage involving or trauma.
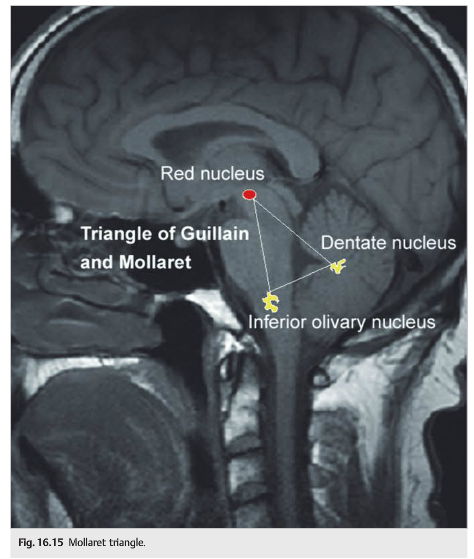
Location The Guillain-Mollaret triangle (the region connecting the red nucleus to the inferior olive and the dentate nucleus.
Treatment The condition may improve with gabapentin, anticholinergic agents, or ceruletide.
20. What are the characteristics, concerns, lesion location, and treatment for oculomasticatory myorhythmia?
Characteristics
Oculomasticatory myorhythmia is defined as pendular nystagmus with pendular convergence and divergence movements of the eyes, with occasional movements of the jaw, face, or limbs.
It is often associated with a supranuclear vertical gaze palsy.
Concerns It is pathognomonic of Whipple disease caused by Tropheryma whippelii. This disorder is a malabsorption syndrome with small intestine involvement; the disease also affects the joints, central nervous system, and cardiovascular system. T whipplei infection is recognized to be a major cause of culture-negative endocarditis
Treatment In the presence of Oculomasticatory Myorhythmia, neither jejunal biopsy nor blood or CSF PCR of Tropheryma whippelii is necessary for the initiation of trimethoprim-sulfamethoxazole.
21. What are the characteristics, concerns, and treatment for Wernicke encephalopathy?
Characteristics
Wernicke encephalopathy is a vitamin B1 deficiency (thiamine).
It presents with the classic triad of ocular findings, cerebellar dysfunction, and confusion.
It occurs most often in the setting of alcoholism). It may produce any type of nystagmus.
Concerns Wernicke encephalopathy should be treated very urgently (vitamin B1 deficiency). It occurs most often in the setting of alcoholism and bariatric surgery).
Treatment Intravenous thiamine should be administered urgently and should be given to any confused patient with nystagmus.
22. Which patterns of jerk nystagmus have localizing/diagnostic value?
1. Downbeat – Cervicomedullary junction, foramen magnum, vestibulocerebellum, and medulla
2. Periodic alternating – Cerebellum, particularly the nodulus and uvula, and by lesions of the cervicomedullary junction
3. Rebound – Cerebellum and medulla (in the region of the nucleus prepositus hypoglossi and medial vestibular nucleus)
4. Brun – Cerebellopontine angle
5. Dissociated jerk – Internuclear ophthalmoplegia (MLF in brainstem)
23. Which patterns of pendular nystagmus have localizing/diagnostic value?
1. Monocular (often vertical) – Visual loss
2. Seesaw – Parasellar lesions and septo-optic dysplasia
3. Oculopalatal myoclonus – Mollaret triangle (connecting red nucleus to inferior olive and dentate nucleus
4. Oculomasticatory myorhythmia – Whipple disease
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
16.1.3 Acquired Nystagmus
Gaze-Evoked Nystagmus
Gaze-evoked is the most common type of nystagmus (see ▶Fig. 16.5).
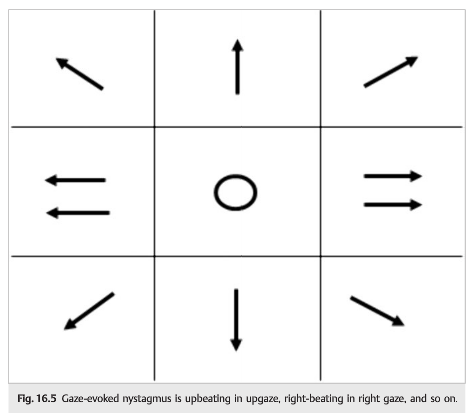
It is absent in the primary position and is not visually disabling. Jerk nystagmus beats in the direction of gaze. It results from impairment in eccentric gaze-holding mechanisms, such as from sedative medications/anticonvulsants and brainstem and cerebellar lesions (central vestibular dysfunction).
Nystagmus with Positional Vertigo
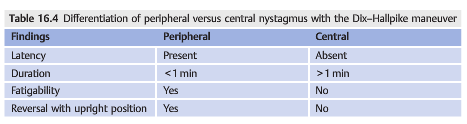
Paroxysmal vertigo occurs only in certain positions. When the Dix–Hallpike maneuver (see ▶Fig. 16.3) is performed, nystagmus is seen (see ▶Table 16.4).
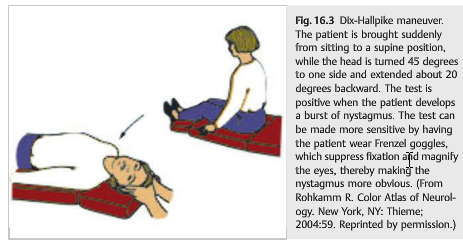
Most patients have benign paroxysmal positional vertigo (BPPV) from a peripheral lesion, usually canalolithiasis or cupulolithiasis in the posterior semicircular canal. BPPV does not respond well to medications but may have a long-term favorable response to numerous maneuvers aimed at dislodging the debris from the posterior semicircular canal. Positional vertigo may also occur with central nervous system disease.
Acquired Central Nystagmus
The most important goal of the evaluation is to identify those patterns of nystagmus that have a localizing value.
Downbeat Nystagmus
Downbeat nystagmus is a type of jerk nystagmus, with the fast phase downward in the primary position (▶Fig. 16.6).

The nystagmus decreases in upgaze and worsens in downgaze; it is usually most prominent in lateral gaze and downgaze. Oscillopsia is usually prominent because the nystagmus is present in primary position and in down-gaze, the preferred reading position.
Downbeat nystagmus is caused by lesions at the cervicomedullary junction, foramen magnum, vestibulocerebellum, and medulla. It is commonly seen in cerebellar degenerations; paraneoplastic syndromes; Chiari malformation (▶Fig. 16.7); encephalitis; trauma; hypomagnesemia; thiamine deficiency; B12 deficiency; and toxicity with lithium, alcohol, amiodarone, toluene, phenytoin, and carbamazepine.

The treatment of downbeat nystagmus is limited. Removal of a toxic drug and treatment of vitamin deficiency may result in improvement. Aminopyridines, clonazepam, valproate, baclofen, and gabapentin may dampen downbeat nystagmus. Patients should be advised to avoid looking down and to not use glasses with bifocal or progressive lenses. Base-down prisms in reading glasses can be used to force the eyes upward.
Upbeat Nystagmus
Upbeat nystagmus is a type of jerk nystagmus with fast phase upward in primary position (▶Fig. 16.8). It often worsens in upgaze.
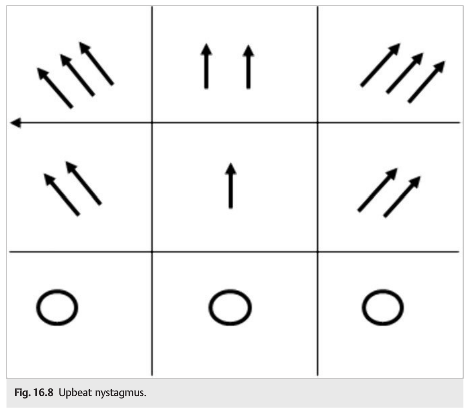
It may be caused by lesions of the medulla, cerebellar vermis, and midbrain and is commonly seen in Wernicke encephalopathy and encephalitis.
Aminopyridines and baclofen may dampen upbeat nystagmus. Patients should avoid looking up and should not use glasses with progressive lenses. Base-up prisms in reading glasses can be used to force the eyes downward.
Periodic Alternating Nystagmus
Periodic alternating nystagmus (PAN) is a type of horizontal jerk nystagmus that alternates direction in primary position (i.e., jerk nystagmus to the right for about 60 to 90seconds, which diminishes, only to begin beating to the left for another 60 to 90seconds) (▶Fig. 16.9). Patients may have a periodic alternating head turn to minimize the nystagmus, and oscillopsia is usually present.
PAN is caused by lesions of the cerebellum, particularly the nodulus and uvula, and by lesions of the cervicomedullary junction. It is commonly seen in multiple sclerosis, cerebellar degenerations (▶Fig. 16.10), Chiari malformations, trauma, hepatic encephalopathy, and albinism, as well as with use of anticonvulsants and lithium. It is responsive to baclofen.

Rebound Nystagmus
Rebound nystagmus is seen in some patients with gaze-evoked nystagmus. It is the reversal of jerk nystagmus direction after sustained eccentric gaze. Rebound nystagmus is caused by cerebellar disorders and lesions of the medulla (in the region of the nucleus prepositus hypoglossi and medial vestibular nucleus).
Brun Nystagmus
Brun nystagmus is a combination of unilateral peripheral vestibular nystagmus from an eighth nerve tumor (▶Fig. 16.11) and gaze-paretic central nystagmus as the tumor compresses the pons. It is characterized by high-frequency, low-amplitude nystagmus on looking away from the lesion, beating in the direction of gaze (due to the vestibular lesion), and low-frequency, high-amplitude horizontal nystagmus on looking toward the lesion, beating in the direction of gaze (due to defective gaze holding). Brun nystagmus is caused by large tumors in the cerebellopontine angle.
Dissociated Jerk Nystagmus
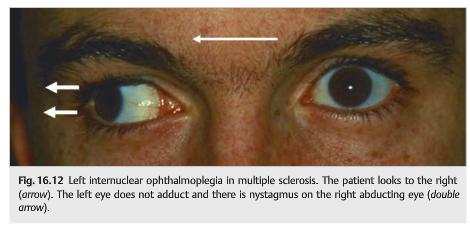
Dissociated jerk nystagmus refers to nystagmus that is different in the two eyes. The most common cause is internuclear ophthalmoplegia (adduction deficit associated with contralateral abducting nystagmus) (▶Fig. 16.12). The abducting nystagmus may be an adaptive mechanism to overcome the adduction paresis.
Acquired Pendular Nystagmus
One of the most common types of nystagmus is acquired pendular nystagmus, which is visually disabling because of severe oscillopsia (▶Fig. 16.2). It most commonly is caused by multiple sclerosis. Oscillopsia may improve with gabapentin, memantine, clonazepam, or valproate.

Seesaw Nystagmus
Seesaw nystagmus (▶Fig. 16.13) is defined as pendular nystagmus with elevation and intorsion of one eye simultaneous with depression and extorsion of the other eye, followed by a reversal of the cycle, so that the eyes move like a seesaw.
Seesaw nystagmus produces very disabling oscillopsia that responds poorly to any treatment. It is most often caused by parasellar lesions and may be seen with pituitary tumors (▶Fig. 16.14), craniopharyngiomas, septo-optic dysplasia, and brainstem lesions (especially in the midbrain).
Oculopalatal Myoclonus (or Tremor)
Oculopalatal myoclonus is a type of vertical pendular nystagmus coexisting with tremor of the palate and/or facial muscles, larynx, and diaphragm. It is present during sleep. It usually develops months after an infarction or hemorrhage involving the Mollaret triangle (the region connecting the red nucleus to the inferior olive and the dentate nucleus; ▶Fig. 16.15) but can also be delayed after trauma to this region. The condition may improve with gabapentin, anticholinergic agents, or ceruletide.
Oculomasticatory Myorhythmia
Oculomasticatory myorhythmia is defined as pendular nystagmus with pendular convergence and divergence movements of the eyes, with occasional movements of the jaw, face, or limbs. It is often associated with a supranuclear vertical gaze palsy and is pathognomonic of Whipple disease.
Pearls
Wernicke encephalopathy (vitamin B1 deficiency-occurs most often in the setting of alcoholism and bariatric surgery) may produce any type of nystagmus. Intravenous thiamine should be given to any confused patient with nystagmus.
16.1.4 Management of Nystagmus
The aim of management is to improve oscillopsia and/or visual blurring. Drug therapy is often empirical; there are usually poor results, except for PAN and some cases of acquired pendular nystagmus. Commonly used medications include the following:
● Baclofen (periodic alternating nystagmus)
● Gabapentin (acquired pendular nystagmus)
● Memantine (acquired pendular nystagmus)
● Aminopyridines (downbeat and upbeat nystagmus)
● Clonazepam
● Valproate
● Trihexyphenidyl or other anticholinergics
Other treatment possibilities are prisms to move the null point into primary position or away from a triggering gaze (i.e., move the eyes up in cases of downbeat nystagmus), or to induce convergence; contact lenses to dampen the nystagmus; eye muscle surgery (Kestenbaum procedure) to move the null point into primary position; and injection of botulinum toxin in the extraocular muscles to immobilize the eye (but this induces diplopia and often requires patching of one eye).
16.4 Summary of the Evaluation of the Patient with Ocular Oscillations (▶Fig. 16.20)
The diagram below summarizes the steps necessary for the characterization of ocular oscillations.

Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.