Questions:
24. What are the characteristics and the lesion location for convergence-retraction nystagmus?
25. What are the characteristics, concerns, and treatment for superior oblique myokymia?
26. What are the characteristics, concerns, and the lesion location for ocular bobbing?
27. What are the characteristics of saccadic intrusions?
28. What are the characteristics and concerns for ocular flutter?
29. What are the characteristics and concerns for opsoclonus?
30. What are the characteristics and concerns for square-wave jerks and macrosquare-wave jerks?
31. What are the characteristics, concerns, and lesion location for ocular dysmetria?
32. What are the characteristics of voluntary nystagmus?
33. What are the characteristics, concerns and lesion location for internuclear ophthalmoplegia?
________________________________________
Questions with answers:
24. What are the characteristics and the lesion location for convergence-retraction nystagmus?
Characteristics
Convergence-retraction nystagmus is a component of the dorsal midbrain syndrome or Parinaud’s syndrome which includes:
convergence-retraction nystagmus,
vertical gaze abnormalities (typically upgaze paresis but sometimes downgaze palsy),
upper eyelid retraction (Collier sign), and
light-near dissociation of the pupils.
Location It is caused by midbrain/posterior commissure lesions.
25. What are the characteristics, concerns, and treatment for superior oblique myokymia
Characteristics
Oscillopsia or intermittent diplopia that is elicited by having the patient look in the direction of the action of the superior oblique muscle.
Monocular, rapid, intorsional movements of one eye.
It is best seen at the slit lamp or with an ophthalmoscope.
Concerns It is usually benign, and no underlying etiology is found.
However, neuroimaging is recommended, looking for posterior fossa tumors.
Treatment Carbamazepine, baclofen, or propranolol.
Surgical weakening of the superior oblique muscle may be performed in refractory cases.
26. What are the characteristics, concerns, and the lesion location for ocular bobbing?
Characteristics
Ocular bobbing is characterized by conjugate eye movements beginning with a fast downward movement, followed by a slow drift back to the midline (similar to a fish bob in the water).
Concerns It is commonly found in comatose patients with a massive pontine lesion or metabolic encephalopathy.
Location Pontine lesions
27. What are the characteristics of saccadic intrusions?
Characteristics
Saccadic intrusions (flutter and opsoclonus) are abnormal rapid eye movements (saccades) that have no slow phase. All such eye movements disrupt fixation and may interfere with vision.
Saccadic oscillations are often mistaken for nystagmus. In contrast to nystagmus, in which there is always a slow-phase eye movement, saccadic oscillations are saccades (rapid refixation eye movements) without any slow phases.
28. What are the characteristics and concerns for ocular flutter?
Characteristics
Ocular flutter is characterized by intermittent bursts of back-to-back horizontal saccades without any interval between saccades.
There is no vertical component.
Bursts of ocular flutter typically last for seconds at a time.
Ocular flutter is strictly horizontal direction which distinguishes it from opsoclonus, and the lack of interval between the saccades distinguishes ocular flutter from square-wave jerks.
Concerns
Causes of ocular flutter and opsoclonus include the following:
1. Paraneoplastic: Neuroblastoma in children: 50% of children with opsoclonus harbor neuroblastoma; 2% of children with neuroblastoma have opsoclonus. Small cell carcinomas, lung & breast cancers associated with anti-Ri antibodies in adults.
2. Encephalitis, cerebellitis.
3. Intracranial tumor, hydrocephalus, thalamic hemorrhage, multiple sclerosis, nonketotic hyperosmolar coma, drug toxicity (lithium, phenytoin, cocaine, amitriptyline, toluene, organophosphates).
4. Antineuronal antibodies: Ri, Yo, Ma1, Ma2, amphiphysin, CV2, CRMP-5. -5. Idiopathic
29. What are the characteristics and concerns for opsoclonus?
Characteristics
Opsoclonus is back-to-back saccades in multiple directions, including horizontal, vertical, and torsional (sometimes referred to as “saccadomanis”).
These movements are higher amplitude and last longer than typical ocular flutter.
Eye movements are often associated with blinking, facial twitching, myoclonus, and ataxia (“dancing eyes and dancing feet”).
Concerns
1. Paraneoplastic: neuroblastoma in children: 50% of children with opsoclonus harbor a neuroblastoma and 2% of children with neuroblastoma have opsoclonus.
2. Small cell carcinomas and other cancers associated with anti-Ri antibodies in adults.
3. encephalitis/cerebellitis,
4. intracranial tumor,
5. hydrocephalus,
6. thalamic hemorrhage,
7. multiple sclerosis,
8. nonketotic hyperosmolar coma,
9. drug toxicity (lithium, phenytoin, and cocaine)
30. What are the characteristics and concerns for square-wave jerks and macrosquare-wave jerks?
Characteristics
Horizontal to-and-fro saccades that interrupt fixation are referred to as square-wave jerks.
Unlike ocular flutter, square-wave jerks have intersaccadic intervals.
They are termed macrosquare-wave jerks when the amplitude is > 5 degrees.
Concerns Common causes include cerebellar diseases, Parkinson disease, and progressive supranuclear palsy.
31. What are the characteristics, concerns and lesion location for ocular dysmetria?
Characteristics
In ocular dysmetria, the eye overshoots (saccadic hypermetria) or undershoots (saccadic hypometria) the target upon refixation.
It then saccades back or forward to the intended fixation point (back-up or catch-up saccade).
Concerns It is a sign of cerebellar dysfunction similar to limb dysmetria.
Location Cerebellum
32. What are the characteristics for voluntary nystagmus?
Characteristics
Some normal subjects can induce ocular oscillations (often with convergence) mimicking ocular flutter accompanied by convergence effort.
The duration of this nystagmus is brief, usually less than 30 seconds.
33. What are the characteristics, concerns, and lesion location for internuclear ophthalmoplegia?
Characteristics
1. variable adduction deficit in the eye ipsilateral to the lesion
2. slowed ipsilateral adducting saccades
3. a contralateral dissociated abducting eye horizontal nystagmus
Concerns
Demyelinating disease in the young and stroke in older patients.
Myasthenia gravis can also mimic the clinical presentation of an INO.
Location In the medial longitudinal fasciculus in the midbrain or pons.
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
16.2 Other Nystagmoid Eye Movements
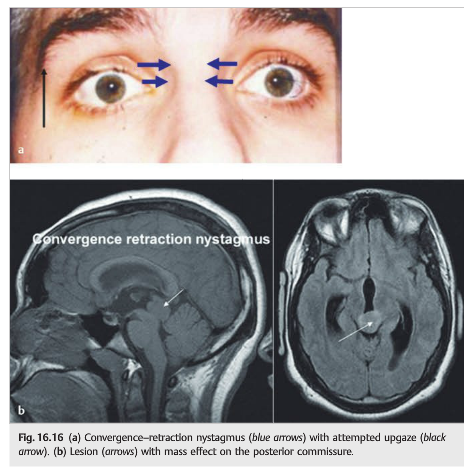
16.2.1 Convergence–Retraction Nystagmus
Convergence–retraction nystagmus (▶Fig. 16.16a) is not truly nystagmus, but rather bilateral adducting saccades causing convergence of both eyes, without any slow phase. It is most often elicited by having the patient attempt to look up, at which time the eyes converge and retract in the orbit. The retraction is best seen by observing the patient from the side. Convergence–retraction nystagmus is one of many signs of Parinaud dorsal midbrain syndrome (upgaze paresis, light-near dissociation of the pupils, and upper eyelid retraction). It is caused by midbrain/posterior commissure lesions (▶Fig. 16.16b).
16.2.2 Superior Oblique Myokymia
Superior oblique myokymia (▶Fig. 16.17) is defined as oscillation of one eye due to intermittent firing of the superior oblique muscle (myokymia or tremor of the superior oblique muscle).
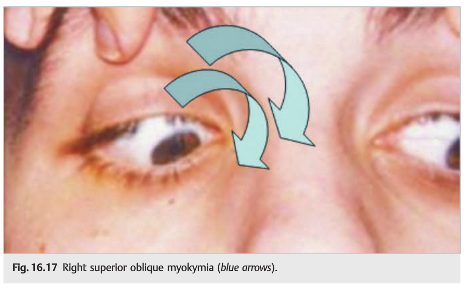
It produces oscillopsia or intermittent diplopia, elicited by having the patient look in the direction of the superior oblique muscle, and is characterized by monocular, rapid, intorsional movements. It is best seen at the slit lamp or with an ophthalmoscope. Superior oblique myokymia is usually benign, and no underlying etiology is found. However, neuroimaging is recommended, looking for posterior fossa tumors. Superior oblique myokymia is usually chronic with periods of remission.
Treatment includes carbamazepine, baclofen, or propranolol. Surgical weakening of the superior oblique muscle may be performed in refractory cases.
16.2.3 Ocular Bobbing
Ocular bobbing is characterized by conjugate eye movements beginning with a fast downward movement, followed by a slow drift back to the midline (similar to a fish bob in the water). It is commonly found in comatose patients with a massive pontine lesion or metabolic encephalopathy.
16.3 Saccadic Intrusions
Saccadic intrusions are often mistaken for nystagmus. In contrast to nystagmus, in which there is always a slow-phase eye movement, saccadic oscillations are saccades(rapid refixational eye movements) without any slow phases.
16.3.1 Ocular Flutter
Ocular flutter (▶Fig. 16.18) is characterized by intermittent bursts of back-to-back horizontal saccades without any interval between saccades. There is no vertical component. Bursts of ocular flutter typically last for seconds at a time. The strictly horizontal direction distinguishes ocular flutter from opsoclonus, and the lack of interval between the saccades distinguishes ocular flutter from square-wave jerks.

16.3.2 Opsoclonus
Opsoclonus is back-to-back saccades in multiple directions, including horizontal, vertical, and torsional (sometimes referred to as “saccadomania”). These movements are higher amplitude and last longer than typical ocular flutter. Eye movements are often associated with blinking, facial twitching, myoclonus, and ataxia (“dancing eyes and dancing feet”).
Causes of Ocular Flutter and Opsoclonus
Causes of ocular flutter and opsoclonus include the following:
● Paraneoplastic:
○ Neuroblastoma in children: 50% of children with opsoclonus harbor a neuroblastoma; 2% of children with neuroblastoma have opsoclonus.
○ Small cell carcinomas and other cancers associated with anti-Ri antibodies in adults
● Encephalitis, cerebellitis
● Intracranial tumor, hydrocephalus, thalamic hemorrhage, multiple sclerosis, nonketotic hyperosmolar coma, drug toxicity (lithium, phenytoin, and cocaine)
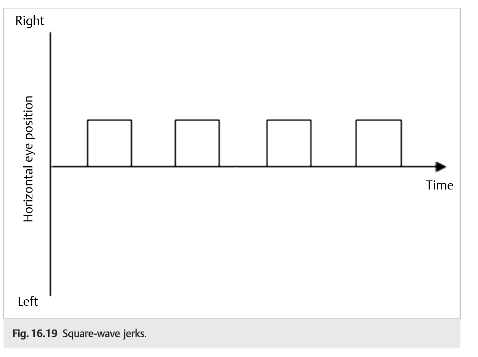
16.3.3 Square-Wave Jerks and Macrosquare-Wave Jerks
Horizontal to-and-fro saccades that interrupt fixation are referred to as square wave jerks (▶Fig. 16.19). Unlike ocular flutter, square-wave jerks have intersaccadic intervals. They are termed macrosquare-wave jerks when the amplitude is>5 degrees. Common causes include cerebellar diseases, Parkinson disease, and progressive supranuclear palsy.
16.3.4 Ocular Dysmetria
In ocular dysmetria, the eye overshoots (saccadic hypermetria) or undershoots (saccadic hypometria) the target upon refixation. It then saccades back or forward to the intended fixation point (back-up or catch-up saccade). It is a sign of cerebellar dysfunction similar to limb dysmetria.
16.3.5 Voluntary Nystagmus
Some normal subjects can induce ocular oscillations (often with convergence and subtle movements of the eyelids such as squinting) mimicking ocular flutter accompanied by convergence effort.
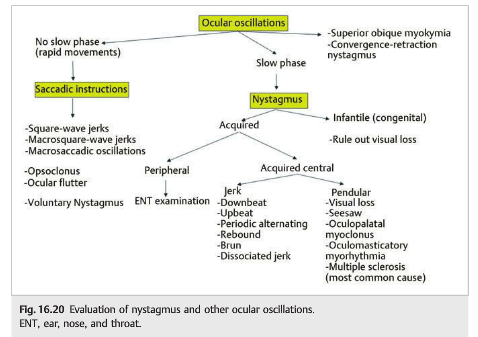
16.4 Summary of the Evaluation of the Patient with Ocular Oscillations (▶Fig. 16.20)
The diagram below summarizes the steps necessary for the characterization of ocular oscillations.
References:
1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
2. Internuclear Ophthalmoplegia. Marcus Toral, Jaclyn Haugsdal, Michael Wall. University of Iowa. EyeRounds.org 2017 http://webeye.ophth.uiowa.edu/eyeforum/cases/252-internuclear-ophthalmoplegia.htm
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.