Questions:
1. What are the findings of the Locked-in Syndrome?
2. Where is the lesion in the Locked-in Syndrome?
3. What is Ocular Neuromyotonia?
4. What are the symptoms of Ocular Neuromyotonia?
5. What is the usual cause of Ocular Neuromyotonia?
6. Where do these findings localize the lesion: Horizontal gaze palsy with ipsilateral facial palsy?
7. Where do these findings localize the lesion: 6th nerve palsy with contralateral hemiparesis (Raymond syndrome)?
8. Where do these findings localize the lesion: 6th nerve palsy with ipsilateral seventh nerve palsy and contralateral hemiparesis (Millard-Gubler syndrome)?
9. Where do these findings localize the lesion: 6th nerve palsy with ipsilateral seventh nerve palsy, deafness, hypoesthesia, Horner syndrome, contralateral pain and thermal hypoesthesia, ataxia (Foville syndrome)?
10. Where do these findings localize the lesion: 6th nerve palsy with ipsilateral Horner Syndrome?
_______________________________________________
Questions with answers:
1. What are the findings of the Locked-in Syndrome?
Quadriplegia, Absence of horizontal eye movements, Mutism, Preservation of vertical eye movements, Normal blinking and Normal consciousness
2. Where is the lesion in the Locked-in Syndrome?
Large bilateral lesions (essentially transecting the pons)
3. What is Ocular Neuromyotonia?
It is tonic spasms of the extraocular muscles innervated by a specific ocular motor nerve (third or sixth cranial nerve) occur during sustained eccentric gaze.
4. What are the symptoms of Ocular Neuromyotonia?
Affected patients complain of episodic diplopia lasting seconds or minutes and occurring after they look in a specific direction for a few seconds. Some patients feel that the eye is pulled in the orbit.
5. What is the usual cause of Ocular Neuromyotonia?
This rare disorder classically develops months or years after radiation involving the ocular motor nerves usually for pituitary tumor or skull base tumor. Carbamazepine is sometimes helpful.
6. Where do these findings localize the lesion: Horizontal gaze palsy with ipsilateral facial palsy?
Pons – 6th nerve nucleus
7. Where do these findings localize the lesion: 6th nerve palsy with contralateral hemiparesis (Raymond syndrome)?
Pons – 6th nerve fascicle and corticospinal tract
8. Where do these findings localize the lesion: 6th nerve palsy with ipsilateral seventh nerve palsy and contralateral hemiparesis (Millard-Gubler syndrome)?
Pons – 6th nerve fascicle, seventh nerve fascicle, and corticospinal tract
9. Where do these findings localize the lesion: 6th nerve palsy with ipsilateral seventh nerve palsy, deafness, hypoesthesia, Horner syndrome, contralateral pain and thermal hypoesthesia, ataxia (Foville syndrome)?
Pons – 6th nerve fascicle or nucleus, ipsilateral seventh nerve fascicle or nucleus, auditory nerve, descending tract of 5th nerve, cerebellar peduncle, and spinothalamic tract
10. Where do these findings localize the lesion: 6th nerve palsy with ipsilateral Horner syndrome?
Cavernous sinus
_______________________________________________
The information below is from Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
13.5.6 Other Eye Movement Abnormalities
Locked-in Syndrome
Large bilateral lesions (essentially transecting the pons) may cause a neurologic state characterized by the combination of the following:
● Quadriplegia
● Absence of horizontal eye movements
● Mutism
● Preservation of vertical eye movements
● Normal blinking
● Normal consciousness
These patients are able to communicate only by using blinking and vertical eye movements.
Ocular Neuromyotonia
In ocular neuromyotonia, tonic spasms of the extraocular muscles innervated by specific ocular motor nerve (e.g., third or sixth cranial nerve) occur during sustained eccentric gaze (hyperaction of the muscle).
Affected patients complain of episodic diplopia lasting seconds or minutes and occurring after they look in a specific direction for a few seconds. Some patients feel that the eye is pulled in the orbit. The examination is usually normal between episodes.
This rare disorder classically develops months or years after radiation involving the ocular motor nerves (usually for pituitary tumor or skull base tumor). Carbamazepine Is sometimes helpful.
Ocular Motility Deficits in High Myopia
Adults with high axial myopia (associated with a long globe) may develop an esotropia, abduction deficit, or vertical misalignment.
Various explanations have been proposed, including the following:
● Elongated Globe (compromising free movements of the eye in the orbit)
● Heavy globe
● Lateral rectus (or its tendon) abnormalities
● Defective orbital connective tissue
● Abnormal insertions of the extraocular muscles
Diplopia after Ocular Surgery
Numerous processes may explain diplopia after ocular surgery.
● Monocular diplopia is common after refractive surgery, cataract surgery, and retinal surgery resulting from any of the following unwanted outcomes:
○ Irregular cornea
○ Incision-induced astigmatism
○ Decentered, tilted intraocular lens
○ Cracked lens○ Problem (fold, tear, opacity) of the posterior capsule
○ Eccentric pupil
○ Iridectomy creating multiple pupils
● Binocular diplopia suggests ocular misalignment, which can occur as a result of the following:
○ Disrupted fusion secondary to
– anisometropia
– surgical pupil changes
– altered brightness sense between the eyes
– prolonged decreased vision in the eye with cataract
– sensory exotropia
○ Decentered or tilted intraocular lens with induced prism
○ Extraocular muscle trauma from local anesthesia (peri- or retrobulbar block)
○ Unmasking of preexisting tropia (the patient sees double because the vision has improved)
○ Impaired eye movement after scleral buckle (retinal detachment repair)
○ Bridle suture sometimes placed on a rectus muscle during surgery
Isolated ptosis after ocular surgery is common, usually related to damage to the levator palpebrae from the speculum used to keep the eye open during surgery.
13.6 Evaluation of the Patient with Binocular Diplopia: Practical Tips
13.6.1 Assessment of Diplopia
● Is the diplopia binocular or monocular?
● If monocular, you are done! Send the patient to an ophthalmologist.
● If binocular:
○ Is it horizontal or vertical?
○ Is it worse at distance or at near?
○ In which direction of gaze is the diplopia worse?
Pearls
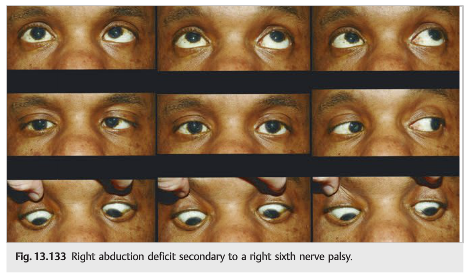
Esotropia (e.g., an abduction deficit) gives diplopia worse at distance (the eyes normally converge at near). Exotropia (e.g., an adduction deficit) gives diplopia worse at near (the eyes normally diverge when looking at distance). The diplopia is worse in the direction of the paretic muscle.
Example: A patient with a right sixth nerve palsy complains of the following (▶Fig. 13.133):
● Binocular diplopia
● Horizontal diplopia
● Worse at distance (the eyes need to diverge at distance)
● Worse when looking to the right
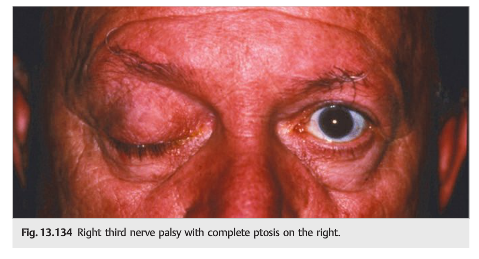
Example: A patient with a complete ptosis and abnormal eye movements may not complain of diplopia until the ptotic eyelid is raised by the examiner (▶Fig. 13.134).
13.6.2 Further Assessment of the Diplopic Patient
● Is there a head tilt? (important in vertical diplopia) or a face turn?
● Review of old photographs to look for head tilt, face turn, or old strabismus.
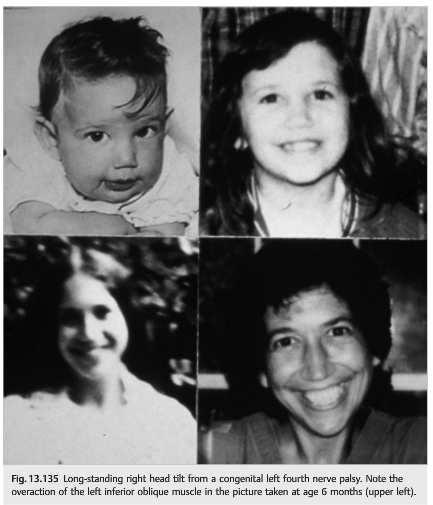
Patients and families are often not aware of head tilt. A long-standing head tilt is best revealed by reviewing old pictures. Example: In a patient with binocular vertical diplopia, a long-standing head tilt is highly suggestive of decompensation of a congenital fourth nerve palsy (patients tilt their head to the opposite side to compensate for the diplopia) (▶Fig. 13.135).
Pearls
Patients often compensate for their diplopia by turning their face or tilting their head (giving the appearance of torticollis). This is particularly common in young children. Eye Movements should be evaluated in children with torticollis.
13.6.3 Look at the Patient
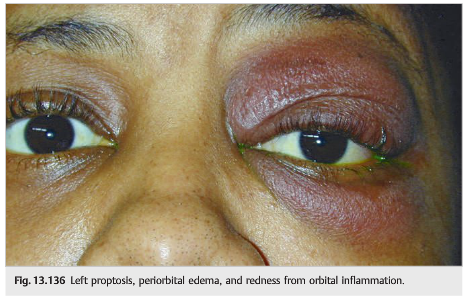
There may be an obvious orbital problem, with red eye or proptosis, alleviating the need for a neurologic evaluation.
Example: The finding of an orbital syndrome (proptosis, periorbital edema, periorbital redness, visual loss) in a patient complaining of diplopia localizes the process to the orbit itself. In this case, the diplopia is usually secondary to dysfunction of the extraocular muscles (▶Fig. 13.136).
13.6.4 Visual Acuity, Pupils, and Fundus Also Need to Be Carefully Examined
● Decreased vision suggests an orbital or an orbital apex process (the visual acuity and visual fields are normal with lesions of the cavernous sinus).
● Bilateral disc edema in the setting of good visual acuity and sixth nerve palsy suggests papilledema secondary to raised intracranial pressure.
● In the evaluation of a third nerve palsy, it is essential to carefully evaluate the pupil.
● A Horner syndrome on the side of a sixth nerve palsy localizes to the cavernous sinus.
Example: A classic cause of unilateral or bilateral sixth nerve palsy is raised intracranial pressure. These patients may have headaches in addition to the binocular horizontal diplopia.
Funduscopic examination needs to be systematically performed in all patients complaining of diplopia. Finding papilledema in the setting of an abduction deficit suggests a sixth nerve palsy from raised intracranial pressure (▶Fig. 13.137).

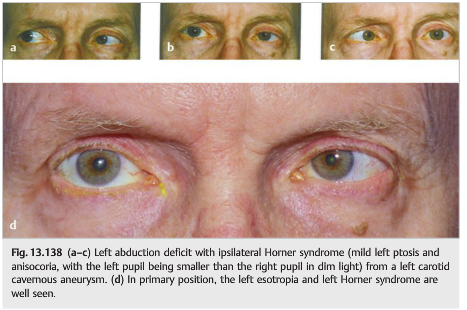
Example: The cavernous sinus is the only place where the sixth nerve is very close to the sympathetic pathway. Therefore, a cavernous sinus lesion can produce a sixth nerve palsy and an ipsilateral Horner syndrome, with no other neurologic signs.
Lesions of the intracavernous carotid artery (such as aneurysm) are particularly common with such a clinical presentation (▶Fig. 13.138).
Example: The pupils are always normal when the extraocular muscles are affected directly (lesion localizing to the muscles), or when the neuromuscular junction is affected (myasthenia gravis).
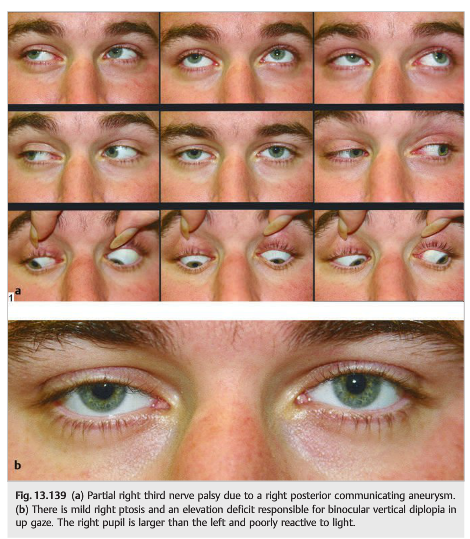
Lesions of the third cranial nerve may produce a mydriasis that reacts poorly to light. Therefore, finding anisocoria, worse in the light, with the large pupil being on the side of a ptosis and abnormal eye movements, is highly suggestive of a third nerve palsy (▶Fig. 13.139).
Pearls
○ Third nerve palsies with pupil involvement need to be evaluated emergently. The two main causes are intracranial aneurysm and pituitary apoplexy.
○ Localization of the lesion is the most important step when evaluating a patient with binocular diplopia. A patient with an isolated abduction deficit of one eye does not necessarily have a sixth nerve palsy. An isolated paresis of the lateral rectus could be due to a disease of the muscle itself, to deficient transmission at the level of the neuromuscular junction (myasthenia), or to a lesion of the cranial nerve (sixth nerve palsy). Associated symptoms and signs often allow localization of the pathological process.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.