Questions:
1. Where is the horizontal gaze center located?
2. What is the location of the burst neurons responsible for horizontal saccades?
3. What are the findings of a lesion of the 6th nerve nucleus?
4. What are the findings of a lesion of the PPRF?
5. What are 4 findings of a unilateral internuclear ophthalmoplegia?
6. Where is the lesion located that produces a unilateral internuclear ophthalmoplegia?
7. What are the findings of a bilateral internuclear ophthalmoplegia?
8. What are the findings of a walleyed bilateral internuclear ophthalmoplegia (WEBINO)?
9. Where is the lesion located that produces a wall-eyed bilateral internuclear ophthalmoplegia (WEBINO)?
10. What are the findings of the One-and-a-Half Syndrome?
11. Where is the lesion located that produces the One-and-a-Half Syndrome?
12. What are 2 common causes of isolated internuclear ophthalmoplegia?
13. What conditions may mimic an isolated internuclear ophthalmoplegia?
14. What conditions may mimic the one-and-a-half syndrome?
____________________________________________________
Questions with answers:
1. Where is the horizontal gaze center located?
The sixth nerve nucleus (also known as the horizontal gaze center) has interneurons that connect to the contralateral third nerve nucleus via the MLF. This allows both eyes to move in the same direction at the same time (e.g., activation of the right sixth nerve nucleus will activate the right lateral rectus innervated by the right sixth nerve, and the left medial rectus innervated by the left third nerve).
2. What the location of the burst neurons responsible for horizontal saccades?
The paramedian pontine reticular formation (PPRF) contains burst neurons responsible for horizontal saccades.
3. What are the findings of a lesion of the 6th nerve nucleus?
Loss of all ipsilateral voluntary and reflexive conjugate eye movements and ipsilateral facial weakness.
4. What are the findings of a lesion of the PPRF?
Loss of all ipsilateral horizontal rapid eye movements (saccades).
5. What are 4 findings of a unilateral internuclear ophthalmoplegia?
1. Deficit of adduction (slowing of adducting saccades) ipsilateral to the lesion
2. Nystagmus of the contralateral abducting eye
3. Skew deviation may be present.
4. Convergence may overcome the adduction deficit
6. Where is the lesion located that produces a unilateral internuclear ophthalmoplegia?
It results from injury to the medial longitudinal fasciculus within the dorsomedial pontine or midbrain tegmentum.
7. What are the findings of a bilateral internuclear ophthalmoplegia?
No adduction of either eye, nystagmus of the abducting eyes and convergence may overcome the adduction deficits.
8. What are the findings of a walleyed bilateral internuclear ophthalmoplegia (WEBINO)?
No adduction of either eye, nystagmus of the abducting eyes (as in a bilateral INO), but the patient is exotropic and there is loss of convergence.
9. Where is the lesion located that produces a wall-eyed bilateral internuclear ophthalmoplegia (WEBINO)?
A rostral lesion within the midbrain may affect the convergence center and bilateral medial longitudinal fasciculus causing bilateral internuclear ophthalmoplegia and divergence.
10. What are the findings of the One-and-a-Half Syndrome?
A gaze palsy to one side, and on attempted gaze to the opposite side impaired adduction and nystagmus of the abducting eye. In addition the patient has a facial palsy on the side with the gaze palsy.
11. Where is the lesion located that produces a One-and-a-Half Syndrome?
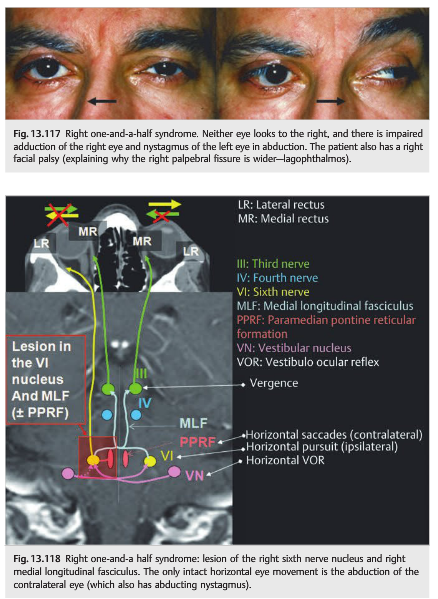
The lesion involves both the abducens nucleus and the medial longitudinal fasciculus. The “one” is an ipsilateral conjugate gaze palsy (lesion of the abducens nucleus) and the “half” is an ipsilateral internuclear ophthalmoplegia (lesion of the MLF). Because the genu of the seventh nerve passes around the 6th nerve nucleus in the facial colliculus, lesions in this area usually result in an ipsilateral peripheral seventh nerve palsy in addition to the conjugate gaze palsy.
12. What are 2 common causes of isolated internuclear ophthalmoplegia?
Multiple sclerosis in the young and lacunar infarction in the elderly.
13. What conditions may mimic an isolated internuclear ophthalmoplegia?
Myasthenia gravis and Wernicke encephalopathy can mimic isolated internuclear ophthalmoplegia.
14. What conditions may mimic the one-and-a-half syndrome?
Myasthenia gravis and Wernicke encephalopathy can mimic isolated the one-and-a-half syndrome.
____________________________________________________
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
13.5.5 The Lesion Is Internuclear or Supranuclear
Internuclear and supranuclear ocular motor disorders are caused by damage to those parts of the brain proximal to the ocular motor nuclei that include pathways controlling eye movement.
They include lesions in the following:
● Brainstem (medulla, pons, and midbrain)
● Cerebellum
● Hemispheres (thalamus, basal ganglia, cerebral hemispheres)
There are separate final common pathways for control of horizontal eye movements (▶Fig. 13.111) and control of vertical eye movements.
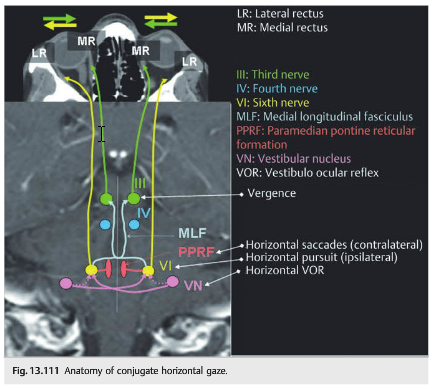
Control of Horizontal Eye Movements
● The sixth nerve nucleus (also known as the horizontal gaze center) has interneurons that connect to the contralateral third nerve nucleus via the MLF. This allows both eyes to move in the same direction at the same time (e.g., activation of the right sixth nerve nucleus will activate the right lateral rectus innervated by the right sixth nerve, and the left medial rectus innervated by the left third nerve).
● The paramedian pontine reticular formation (PPRF) contains burst neurons responsible for horizontal saccades only.
● Each Vestibular nuclear complex sends axons to the ipsilateral (inhibitory) and contralateral (excitatory) sixth nerve nuclei to stabilize the conjugate gaze.
Horizontal Eye Movement Abnormalities
Abnormal horizontal eye movements include the following:
Horizontal Gaze Paresis
A lesion in the pons is the most common location for a horizontal gaze deficit.
● Lesion of the sixth nerve nucleus (▶Fig. 13.112 and ▶Fig. 13.113)
○ Loss of all ipsilateral voluntary and reflexive conjugate eye movements
○ Ipsilateral facial weakness
● Lesion of the PPRF
○ Loss of all ipsilateral horizontal rapid eye movements (saccades)
○ Vestibulo-ocular reflexes and pursuit eye movements are spared with lesions of the PPRF
Classic causes of horizontal gaze paresis include the following:
● Lesions of the pons
○ Infarction (anterior cerebellar artery syndrome)
○ Hemorrhage (vascular malformations)
○ Multiple sclerosis
○ Tumor (glioma, metastasis)
○ Abscess
○ Central pontine myelinolysis
● Wernicke encephalopathy
● Gaucher disease
● Congenital diseases:
○ Bilateral Duane syndrome
○ Möbius syndrome
○ Horizontal gaze palsy with progressive scoliosis (HGPPS)
Internuclear Ophthalmoplegia
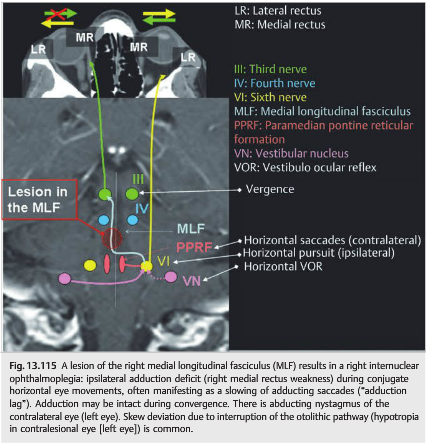
A lesion of the MLF causes an internuclear ophthalmoplegia (INO).
Unilateral INO (▶Fig. 13.114 and ▶Fig. 13.115) consists of the following:
● Ipsilesional deficit of adduction (slowing of adducting saccades)
● Nystagmus of the contralateral abducting eye
● Skew deviation
● Convergence may overcome the adduction deficit
Bilateral Internuclear Ophthalmoplegia (▶Fig. 13.116)



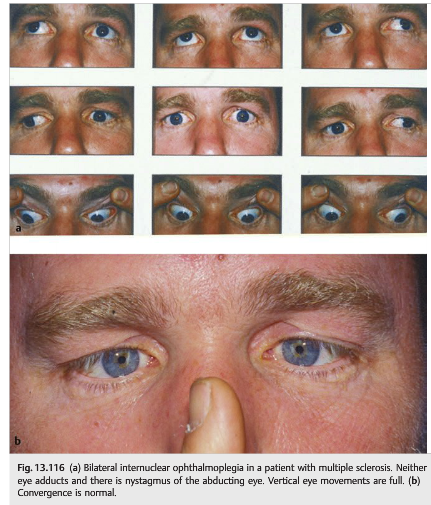
Bilateral internuclear ophthalmoplegia includes the following:
● No adduction of either eye (or slow adducting saccades bilaterally)
● Nystagmus of abducting eyes
● Convergence may overcome the adduction deficits.
● Walleyed bilateral INO (WEBINO): same as already described, but the patient is exotropic and there is loss of convergence
Classic causes of unilateral or bilateral ophthalmoplegia include the following:
● Lesions involving the MLF
○ Multiple sclerosis
○ Infarction (lacune)
○ Hemorrhage (vascular malformations)
○ Tumor (glioma, metastasis)
○ Abscess
○ Central pontine myelinolysis
● Wernicke encephalopathy
Pearls
Bilateral internuclear ophthalmoplegia is a classic finding in patients with multiple sclerosis.
One-and-a-Half Syndrome
Lesions involving both the abducens nucleus and the MLF cause a “one-and-a-half” syndrome (▶Fig. 13.117 and ▶Fig. 13.118):
● The “one” is an ipsilateral conjugate gaze palsy (lesion of the abducens nucleus)
● The “half” is an ipsilateral internuclear ophthalmoplegia (lesion of the MLF)
Classic causes of one-and-a-half syndrome are as follows:
● Lesions involving the pons
○ Infarction (lacuna)
○ Hemorrhage (vascular malformations)
○ Multiple sclerosis
○ Tumor (glioma, metastasis)
○ Abscess
○ Central pontine myelinolysis
● Wernicke encephalopathy
Pearls
○ Common causes of isolated internuclear ophthalmoplegia and one-and-a-half syndrome include multiple sclerosis in the young and lacunar infarction in the elderly.
○ Myasthenia gravis can mimic isolated internuclear ophthalmoplegia and one-and-a-half syndrome.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions and corrections to tcooper@stanford.edu.