Teaching NeuroImages: Upright-supine test to evaluate vertical diplopia
Nailyn Rasool and Sashank Prasad
Neurology May 12, 2015; 84 (19)
RESIDENT AND FELLOW SECTION
Article:
A 36-year-old woman presented with vertical diplopia, nausea, and disequilibrium. Maddox rod testing was performed in the upright and supine positions (figures 1 and 2).
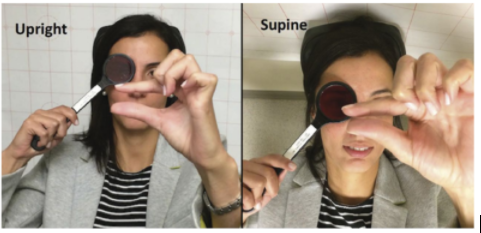
Figure 1 Upright-supine test
During Maddox rod testing, the patient used her fingers to demonstrate the separation of images.
The vertical deviation decreased substantially (over 50%) when supine compared to upright.
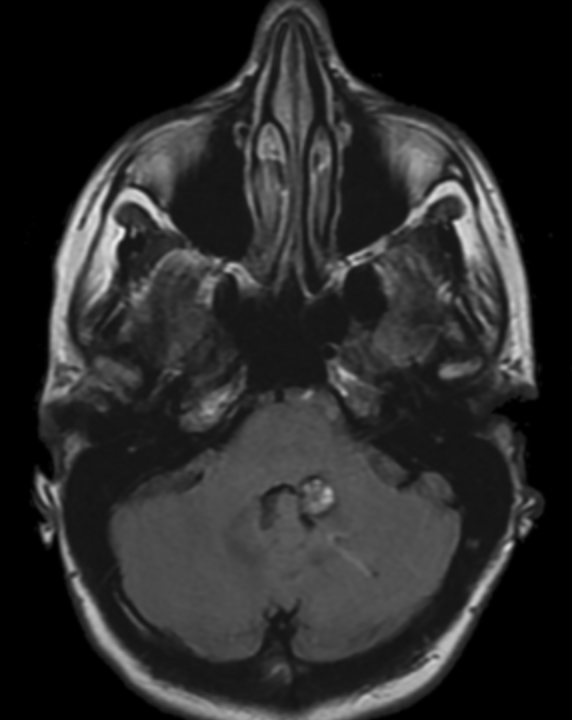
Figure 2 MRI brain (axial fluid-attenuated inversion recovery)
Axial fluid-attenuated inversion recovery MRI demonstrates heterogeneous hyperintensity with a rim of hypointensity, suggestive of a cavernous malformation in the left middle cerebellar peduncle.
Skew deviation is a vertical misalignment caused by a supranuclear lesion in the vertical vestibulo-ocular reflex pathways, including the vestibular nerve, brainstem, or cerebellum. It arises from perturbed utricular inputs, and the amplitude of the ocular deviation is therefore sensitive to gravitational forces.
1 The upright-supine test helps localize the cause of vertical diplopia by distinguishing skew deviation from infranuclear causes.
2 With skew deviation, the vertical deviation is substantially reduced when the patient is supine, whereas with infranuclear lesions it is not.
AUTHOR CONTRIBUTIONS
Nailyn Rasool: drafting/revising the manuscript, study concept or design, analysis or interpretation of data, accepts responsibility for conduct of research and final approval. Sashank Prasad: drafting/revising the manuscript, study concept or design, analysis or interpretation of data, accepts responsibility for conduct of research and final approval, study supervision.
STUDY FUNDING No targeted funding reported.
DISCLOSURE The authors report no disclosures relevant to the manuscript.
REFERENCES
1. Suzuki JI, Tokumasu K, Goto K. Eye movements from single utricular nerve stimulation in the cat. Acta Otolaryngol 1969;68:350–362.
2. Wong AM, Colpa L, Chandrakumar M. Ability of an upright-supine test to differentiate skew deviation from other vertical strabismus causes. Arch Ophthalmol 2011;129:1570–1575.