NOI13 Diplopia 5 – 6th Nerve Palsy
Questions:
1. Where is the nucleus of the 6th cranial nerve located?
2. Which cranial nerve passes through theDorellocanal beneath the petroclynoid (Gruber) ligament?
3. What are the clinical findings of a unilateral 6th nerve nuclear lesion?
4. Why does a unilateral nuclear 6th nerve palsy cause an ipsilateral horizontal gaze palsy?
5. Why is a unilateral 6th nerve palsy often accompanied by an ipsilateral 7th nerve palsy?
6. Where does an ipsilateral Horner syndrome and 6th nerve palsy localize the lesion?
7. Where does an ipsilateral Horner syndrome and 6th nerve palsy associated with a third, fourth, V1 and V2 deficit localize?
8. A microvascular 6th nerve palsy is suspected because a 60-year-old patient has diabetes, hypertension and hyperlipidemia, what tests should be done?
9. A presumed microvascular 6th nerve palsy is suspected in a 60-year-old patient with diabetes, hypertension and hyperlipidemia has not resolved within 3-6 months, what test should be ordered?
10. What is Brown syndrome?
11. What explains the findings of Duane syndrome?
12. What are the findings of Duane syndrome?
13. Are systemic associations common in Duane syndrome?
14. What is the Möbius syndrome?
15.What should be done in a patient with bilateral 6th nerve palsies and a normal MRI?
16. What is best initial imaging study for an isolated 6th nerve palsy in 20-year-old?
17. What is the best initial treatment for a comitant small-angle 6th nerve palsy?
18. What is the likelihood that an isolated,vasculopathic6th nerve palsy will recover?
19. What condition does convergence spasm mimic?
20. What are the findings of convergence spasm?
21. What exam technique should be used in suspected bilateral or unilateral 6th nerve palsy to eliminate convergence spasm?
22. What may mimic a 6th nerve palsy?
____________________________________________________
Questions with answers:
1. Where is the nucleus for the 6th cranial nerve located?
It is located at the medial dorsal pontomedullary junction, near the genu of the seventh nerve.
2. Which cranial nerve passes through theDorellocanal beneath the petroclinoid (Gruber) ligament?
The 6th nerve.
3. What are the clinical findings of a unilateral 6th nerve nuclear lesion?
A sixth nerve nuclear lesion causes an ipsilateral horizontal gaze palsy (neither eye can look in the direction of the lesion). Because the genu of the facial nerve (seventh cranial nerve) passes around the sixth nerve nucleus in the facial colliculus, lesions in this area usually result in an ipsilateral peripheral seventh nerve palsy in addition to the conjugate gaze palsy (facial colliculus syndrome). The inability to move the eyes past the midline horizontally cannot be overcome by the oculocephalic (doll’s head)maneuver or caloric testing
4. Why does a unilateral nuclear 6th nerve palsy cause an ipsilateral horizontal gaze palsy?
The sixth cranial nerve nucleus has two populations of neurons:
a. the abducens motor neurons innervate the ipsilateral lateral rectus muscle.
b. the abducens internuclear neurons which decussate at the level of the sixth cranial nerve nucleus, travel up the MLF, and to the medial rectus subnucleus of the contralateral third cranial nerve. Hence, a lesion of the sixth cranial nerve nucleus causes ipsilateral horizontal gaze palsy.
5. Why is a unilateral 6th nerve palsy often accompanied by an ipsilateral 7th nerve palsy?
Because the genu of the 7th nerve passes around the 6th nerve nucleus in the facial colliculus, lesions in this area usually result in an ipsilateral peripheral seventh nerve palsy in addition to the horizontal gaze palsy.
6. Where does an ipsilateral Horner syndrome and 6th nerve palsy localize the lesion?
In the ipsilateral cavernous sinus.
7. Where does an ipsilateral Horner syndrome and 6th nerve palsy associated with a third, fourth, V1 and V2 deficit localize?
In the cavernous sinus or orbital apex.
8. A microvascular 6th nerve palsy is suspected because a 60-year-old patient has diabetes, hypertension and hyperlipidemia, what tests should be done?
Microvascular 6th nerve palsies are most often nonarteritic but giant cell arteritis should always be considered in patients over 50. Obtain CBC, platelets, ESR and CRP.
9. A presumed microvascular 6th nerve palsy is suspected in a 60-year-old patient with diabetes, hypertension and hyperlipidemia has not resolved within 3-6 months, what tests should be ordered?
Neuroimaging – MRI Brain with and without contrast to rule-out a mass lesion.
10. What is Brown syndrome?
Brown syndrome is an elevation deficit of the affected eye secondary to restriction of the superior oblique tendon. The eye does not elevate when the eye is in adduction (there is a downshoot of the eye in adduction). Brown syndrome may be congenital or acquired.
11. What explains the findings of Duane syndrome?
Duane syndrome is the result of congenital agenesis of the 6th nerve with resultant abnormal innervation of the lateral rectus muscle by branches from the 3rd nerve.
12. What are the findings of Duane syndrome?
a. Unilateral or bilateral marked limitation of abduction and variable limitation of adduction.
b. There is globe retraction and narrowing of the palpebral fissure on attempted adduction secondary to co-contraction of the medial and lateral rectus muscles.
c. Patients usually do not complain of diplopia and are not amblyopic.
13. Are systemic associations common in Duane syndrome?
Yes, systemic associations are present in 30 to 50% (deafness and Goldenhar syndrome are the most common). It occurs more commonly in women and in the left eye. Most cases are sporadic.
14. What is the Möbius syndrome?
A sporadic congenital agenesis of the sixth and seventh nerve nuclei. This results in congenital facial diplegia and bilateral horizontal gaze palsy. It may be accompanied by atrophy of the tongue, deformities of the head and face, endocrine abnormalities, and malformations of the chest, great vessels, and extremities.
15. What should be done in a patient with bilateral 6th nerve palsies and a normal MRI?
Bilateral 6th nerve palsies with normal MRI should have a lumbar puncture with CSF opening pressure and CSF analysis.
16. What is the best initial imaging study for an isolated 6th nerve palsy in a 12-year-old?
Head MRI w&w/o contrast
17. What is the best initial treatment for a comitant small-angle 6th nerve palsy?
Base-out prisms to correct the small-angle deviation.
18. What is the likelihood that an isolated, vasculopathic 6th nerve palsy will recover?
Over 2/3rds of patients recover within 6 months. About 1/3rd will have a recurrence. Patients with bilateral involvement, progression, persistence, or recurrence require neuroimaging.
19. What condition does convergence spasm mimic?
Convergence spasm is often misinterpreted as unilateral or bilateral sixth nerve palsy.
20. What are the findings of convergence spasm?
Both eyes are converged toward the nose, and there is pupillary constriction and lens accommodation (so-called spasm of the near triad).
21. What exam technique should be used in suspected bilateral or unilateral 6th nerve palsy to eliminate convergence spasm?
Ductions should then be tested with each eye covered. Usually, the patient is able to move the eye laterally, and disruption of the near triad will be associated with pupillary dilation as the near triad is released; the pupils constrict again when the patient converges.
22. What may mimic a 6th nerve palsy?
Not all patients with an abduction deficit have a sixth nerve palsy (disorders of the muscle and myasthenia can also give an isolated abduction deficit).
________________________________________________
The information below is from: Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
13.5.3 The Lesion Involves a Cranial Nerve
The diagnosis and management of ocular motor cranial nerve dysfunction vary according to the age of the patient, characteristics of the cranial nerve palsy, and presence of associated symptoms and signs.
Sixth Cranial Nerve (Abducens Nerve) Palsies
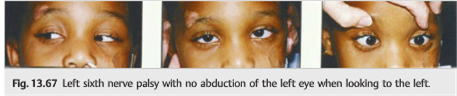
A sixth nerve palsy results in paresis of abduction of the ipsilateral eye and gives binocular horizontal diplopia. Patients with a sixth nerve palsy describe binocular horizontal diplopia that is worse looking toward the side of the sixth nerve palsy. The sixth nerve originates in the pons, close to the facial nerve nucleus. It is often affected by meningeal processes and raised intracranial pressure.
A sixth nerve palsy results in paresis of abduction of the ipsilateral eye (▶Fig. 13.67).
Anatomy of the Sixth Cranial Nerve (▶Fig. 13.68)
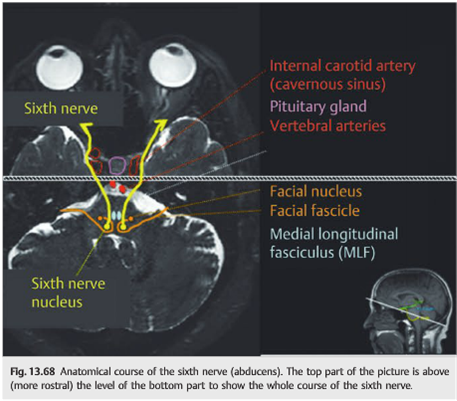
The sixth cranial nerve has a long intracranial course:
● The nucleus is located at the medial dorsal pontomedullary junction, near the genu of the seventh (facial) nerve (facial colliculus area).
● From the sixth nerve nucleus, motor neuron axons traverse anteriorly within the sixth nerve fascicle, whereas interneurons cross over to ascend within the contralateral medial longitudinal fasciculus (MLF) to the medial rectus subnucleus of the third nerve.
● Motor neuron axons exit the pons anteriorly as the sixth nerve.
● The sixth nerve then ascends along the ventral aspect of the brainstem in the subarachnoid space.
● It passes through the Dorello canal beneath the petroclinoid (Gruber) ligament.
● The nerve then enters the cavernous sinus where it is freely situated, lateral to the internal carotid artery. There, it is in close relationship with the sympathetic fibers.
● It enters the orbit through the superior orbital fissure and annulus of Zinn.
● It then innervates the ipsilateral lateral rectus muscle.
Causes of Sixth Cranial Nerve Palsies (▶Table 13.3)
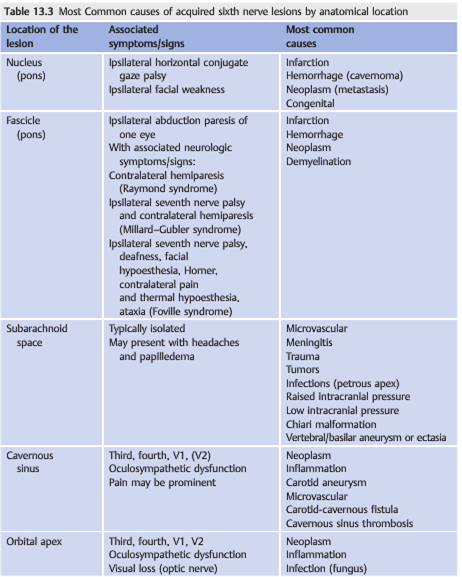
●A sixth nerve nuclear lesion causes an ipsilateral horizontal gaze palsy (neither eye can look in the direction of the lesion). Because the genu of the facial nerve (seventh cranial nerve) passes around the sixth nerve nucleus in the facial colliculus, lesions in this area usually result in an ipsilateral peripheral seventh nerve palsy in addition to the conjugate gaze palsy (facial colliculus syndrome). The inability to move the eyes past the midline horizontally cannot be overcome by the oculocephalic (doll’s head)maneuver or caloric testing (▶Fig. 13.69)

● Because the sixth nerve lies freely within the cavernous sinus, rather than residing within the lateral wall, it may be particularly susceptible to compression in this location by tumor or aneurysm.
● Unilateral or bilateral sixth nerve palsies occur as false localizing signs of supratentorial mass lesions, edema, hemorrhage, or other causes of increased intracranial pressure. Within the subarachnoid space, the nerve is particularly vulnerable to downward pressure on the brainstem as it ascends the ventral aspect of the pons, passes beneath the petroclinoid ligament, and travels over the edge of the tentorium. This appears to be the mechanism of sixth nerve palsies resulting from increased intracranial pressure. For the same reason, hypotension of the cerebrospinal fluid(CSF) (after trauma with CSF leakage, post lumbar puncture, or spontaneous occurrence) can also cause a unilateral or bilateral sixth nerve palsy. All causes of meningitis (infectious, inflammatory, neoplastic) are frequently associated with unilateral or bilateral sixth nerve palsy.
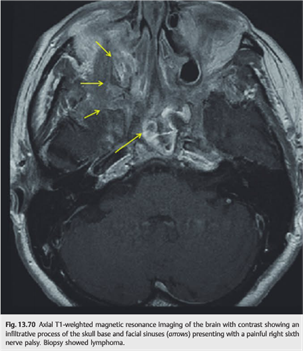
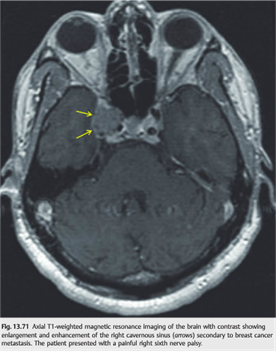
● Lesions of the petrous apex are a classic cause of ipsilateral sixth nerve palsy, most often associated with pain. Because of its relationship with the mastoid, infections are common causes (Gradenigo syndrome). Cerebral venous thrombosis extending to the petrosal sinuses can also produce a sixth nerve palsy. Skull base and cavernous sinus lesions commonly involve the sixth nerve. They may be difficult to see on routine brain MRI and will be easily missed if the MRI scan is performed without contrast (▶Fig. 13.70 and ▶Fig. 13.71).
● An isolated sixth nerve palsy occurring in a patient older than 50 and with atheromatous vascular risk factors is often a microvascular sixth nerve palsy.
Microvascular sixth nerve palsies are secondary to ischemia of the sixth cranial nerve (fascicle or subarachnoid space).
● The onset is acute or rapidly progressive.
● The sixth nerve palsy is isolated.
● Moderate pain over the brow or of the ipsilateral face or head is common.
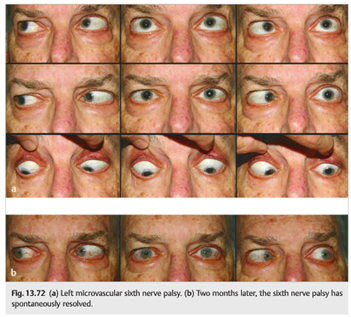
● The sixth nerve palsy almost always resolves completely within 3 to 6 months (▶Fig. 13.72).
Pearls
● Microvascular sixth nerve palsies are most often nonarteritic, but giant cell arteritis should always be considered.
● A microvascular sixth nerve palsy should resolve within 3 to 6 months. Persistent Abduction deficit should prompt an extensive workup.
Rarely, a microvascular sixth nerve palsy may be arteritic, related to vasculitis (especially giant cell arteritis) (▶Fig. 13.73). 
Diplopia in a patient over 50 should raise the possibility of giant cell arteritis.
● Always look for other symptoms or signs of giant cell arteritis.
● Obtain complete blood count (CBC), platelets, C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR).
● The sixth nerve palsy may be subtle with apparently full ductions. The cross-cover test (or the red glass or Maddox rod test) shows an esotropia, which may be comitant. This is particularly common with raised intracranial pressure or Chiari malformations (▶Fig. 13.74).

Chiari malformations often produce neuro-ophthalmic symptoms and signs (▶Fig. 13.75):
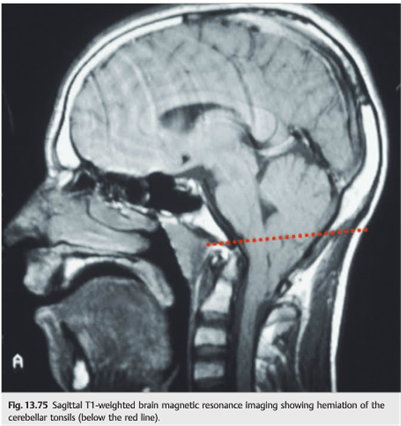
● Headache (often with exercise)
● Dizziness
● Diplopia from unilateral or bilateral sixth nerve palsy or from “divergence insufficiency”
● Downbeat nystagmus
● Raised intracranial pressure with papilledema (rare)
Congenital Sixth Cranial Nerve Palsies
Duane Syndrome
● There is marked limitation of abduction and variable limitation of adduction.
● This is explained by congenital agenesis of the sixth nerve with resultant abnormal innervation of the lateral rectus muscle by branches from the third nerve.
● There is globe retraction and narrowing of the palpebral fissure on attempted adduction secondary to co-contraction of the medial and lateral rectus muscles.
● Duane syndrome can be unilateral or bilateral.
● It occurs more commonly in women and in the left eye.
● Most cases are sporadic.
● Patients usually do not complain of diplopia and are not amblyopic.
● There are systemic associations in 30 to 50% (deafness and Goldenhar syndrome are the most common).
There are three types of Duane syndrome:
● Type I: Limited abduction (most common; patient appears esotropic) (▶Fig. 13.76)

● Type II: Limited adduction (patient appears exotrolpic)
● Type III: Limited abduction and adduction
Möbius Syndrome
● Congenital agenesis of the sixth and seventh nerve nuclei
● Congenital facial diplegia associated with bilateral horizontal gaze palsy
● May be accompanied by atrophy of the tongue, deformities of the head and face, endocrine abnormalities, and malformations of the chest, great vessels, and extremities
● Sporadic
Horizontal Gaze Paresis and Progressive Scoliosis (HGPPS)
● Autosomal recessive
● Congenital absence of horizontal conjugate eye movements with progressive scoliosis during early childhood
Causes of Sixth Cranial Nerve Palsies in Children
Cranial nerve palsies in children differ in frequency from what is classically observed in adults:
● Congenital sixth nerve palsies are common.
○ Cycloplegic refraction is important in children with esotropia: uncorrected hyperopia often results in accommodative esotropia.
○ Congenital esotropia is also common.
○ Duane syndrome is common.
● Acquired sixth nerve palsies are most commonly due to the following:
○ Trauma
○ Posterior fossa tumors
○ Meningitis
○ Raised intracranial pressure (hydrocephalus)
Mimickers of Sixth Cranial Nerve Palsies
Pearls
Not all patients with an abduction deficit have a sixth nerve palsy (disorders of the muscle and myasthenia can also give an isolated abduction deficit).
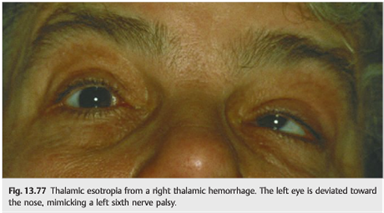
Thalamic Esotropia
● Thalamic lesions can rarely induce convergence of one or both eyes (a contralateral decrease in the normal inhibition of the medial rectus muscle), thereby mimicking unilateral or bilateral sixth nerve palsy.
● Thalamic esotropia is usually associated with up gaze deficits (▶Fig. 13.77).
Convergence Spasm
● Convergence spasm is often misinterpreted as unilateral or bilateral sixth nerve palsy.
● Both eyes are converged toward the nose, and there is pupillary constriction and lens accommodation (so-called spasm of the near triad).
● When the patient is asked to look to each side, the eyes do not move.
● Ductions should then be tested with each eye covered. Usually, the patient is able to move the eye laterally, and disruption of the near triad will be associated with pupillary dilation as the near triad is released; the pupils constrict again when the patient converges (▶Fig. 13.78).

Evaluation of the Patient with Suspected Sixth Cranial Nerve Palsy
● Based on other illnesses and age
● Neurological evaluation looking for other symptoms or signs
● Ophthalmological evaluation looking for orbital syndrome, optic neuropathy, papilledema, other ocular motor cranial nerve involvement
● Systemic evaluation looking for giant cell arteritis (if over 50 years of age), fever, systemic inflammatory disorder, atheromatous vascular risk factors
● Could it be myasthenia?
● Is the sixth nerve palsy isolated, or not?
● Is the sixth nerve palsy painful, or not?
Patients with Isolated sixth nerve palsy may need the following evaluation:
● Patient older than 50 years: CBC, platelets, CRP, ESR, glucose, lipid profile
● MRI of brain and orbits with fat suppression and gadolinium with special attention to the course of the sixth nerve: pons, clivus, petrous area, cavernous sinus, pituitary gland, facial sinus, mastoid, orbital apex, and orbit (rectus muscles and superior orbital vein)
● Magnetic resonance angiography (MRA) or computed tomographic angiography
● (CTA) of the circle of Willis only if a vascular process (aneurysm or carotid cavernous fistula) is suspected
● Lumbar puncture with CSF opening pressure and CSF analysis if MRI is normal and raised intracranial pressure (headache and/or papilledema) or a meningeal processare are suspected
● Bilateral sixth nerve palsies with normal MRI should have a lumbar puncture with CSF opening pressure and CSF analysis. Beware of the possibility of low CSF pressure (spontaneous CSF hypotension).
Although it is not always necessary to obtain an MRI scan in patients with suspected microvascular sixth nerve palsy, most patients undergo imaging. It is, however, also reasonable to observe such patients for recovery, and to obtain imaging only if their abduction deficit persists after 3 months.
Reference: 1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.