Questions:
1. What 5 anatomical components of eye movement can cause binocular diplopia?
2. What holds the image steady during brief head movements?
3. What holds the image steady during sustained head movements?
4. What is Sherrington’s law?
5. What is Hering’s Law?
6. What 2 processes cause most incomitant strabismus?
7. What is the primary deviation in incomitant strabismus?
8. What is the secondary deviation in incomitant strabismus?
9. In incomitant strabismus, is the primary or secondary deviation larger?
10. Does a phoria or a tropia have more value in localizing the defect in a patient with new onset binocular diplopia
11. What is the difference between terms “ocular motor” and “oculomotor”?
12. What is the difference between ductions, versions and vergences?
13. What 3 techniques can help determine if an ocular misalignment is due to a restriction or paresis?
____________________________________________________
Questions with answers:
1. What 5 anatomical components of eye movement can cause binocular diplopia?
a. the extraocular muscles
b. the neuromuscular junction
c. the ocular motor cranial nerves
d. internuclear pathways
e. supranuclear pathways
2. What holds the image steady during brief head movements?
The vestibulo-ocular reflex.
3. What holds the image steady during sustained head movements?
The optokinetic reflex.
4. What is Sherrington’s law?
Sherrington’s law of reciprocal innervation states that when a muscle contracts, its direct antagonist relaxes to an equal extent allowing smooth movement.
5. What is Hering’s Law?
Hering’s law of equal innervation states that during conjugate eye movements, the paired yoke muscles of each eye receive equal innervation so that the eyes move together.
6. What 2 processes cause most incomitant strabismus?
Paralytic and mechanical restrictive processes.
7. What is the primary deviation in incomitant strabismus?
The amount of misalignment when the normal eye is fixating in primary position.
8. What is the secondary deviation in incomitant strabismus?
The amount of misalignment when the paretic eye is fixating in primary position.
9. In incomitant strabismus, is the primary or secondary deviation larger?
The secondary deviation.
10. Does a phoria or a tropia have more value in localizing the defect in a patient with new onset binocular diplopia?
They both have the same value.
11. What is the difference between terms “ocular motor” and “oculomotor”?
Ocular motor nerves are all three cranial nerves involved in ocular movements. The oculomotor refers to the only the 3rd cranial nerve.
12. What is the difference between ductions, versions, and vergences?
Ductions are monocular eye movements.
Versions are binocular conjugate eye movements. Examples: saccades and pursuit movements, oculocephalic responses and vestibulo-ocular reflex (VOR), and optokinetic nystagmus
Vergences are binocular dysconjugate movements in which the two eyes move in opposite directions (the eyes need to converge to see a single image at near, and need to diverge to see a single image at distance).
13. What 3 techniques can help determine if an ocular misalignment is due to a restriction or paresis?
a. Forced duction
b. Measuring the intraocular pressure with eye movement
c. Assessing the velocity of eye movements.
Explanation: “13 Diplopia
The goal of all normal eye movements is to place and maintain an object of visual interest on each fovea simultaneously to allow visualization of a single, stable object. Any deviation from normal eye movement will degrade vision and will often give the perception of double vision (diplopia). Diplopia is a common complaint and often reveals an underlying neurologic disorder.
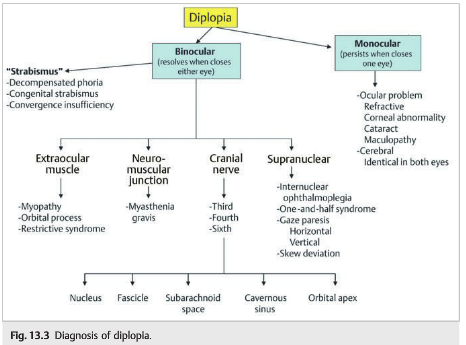
The first step in evaluating a patient who is complaining of diplopia is to determine whether the diplopia is monocular (persists when the patient closes one eye) or binocular (resolves when the patient closes either eye).
13.1 Monocular Diplopia
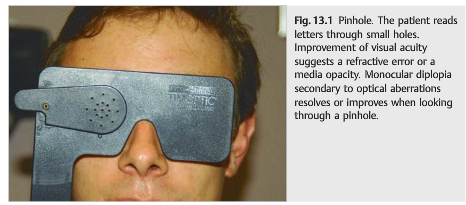
Monocular diplopia is not related to a neurologic disorder and usually results from an optical problem (e.g., abnormal diffraction of light within the eye). It is almost always secondary to an ocular disease (e.g., cataract) or a refractive problem (e.g., astigmatism or issues with glasses).
It is typically alleviated when the patient looks through a pinhole (opaque panel perforated with one or multiple holes of 1 to 1.5mm diameter). The holes restrict incoming light rays to a narrow path that bypasses refractive irregularities and presents a single, focused image to the retina. If monocular diplopia is due to an optical problem, the pinhole will usually make the secondary images disappear (▶Fig. 13.1).
Any uncorrected refractive error or media opacity may be responsible for monocular diplopia. Not all refractive errors can be fully corrected with glasses. In cases of monocular diplopia, correction with contact lenses should be tried.
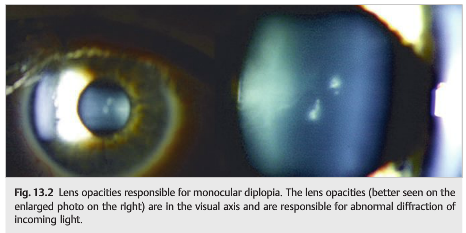
Lens opacities in the visual axis are a common cause of monocular diplopia, which resolves after cataract surgery (▶Fig. 13.2).
Other causes of monocular diplopia include corneal surface irregularity (e.g. ,irregular astigmatism from pterygium or keratoconus, corneal edema, corneal scar, problem with contact lens, dry eye syndrome), post–cataract surgery (e.g., eccentric implant, tilted implant, multifocal implant, posterior capsular opacification), and retinal surface irregularity (e.g., macular edema, epiretinal membrane).
Damage to the visual association areas may very rarely produce duplicative images. In this case, the monocular diplopia or polyopia is present in both eyes (the patient sees double with either eye covered) and is identical in both eyes. Cerebral monocular diplopia is often monocular polyopia (i.e., more than two images).
Monocular diplopia or polyopia from cerebral lesions, however, is rarely an isolated finding; homonymous visual field defects are usually present, and other higher-order visual deficits such as alexia, prosopagnosia, and visual agnosia may be noted (see Chapters 10 and 11).
13.2 Binocular Diplopia
When the diplopia is binocular, it results from ocular misalignment secondary to dysfunction of the extraocular muscles, neuromuscular junction, ocular motor cranial nerves, or the internuclear and supranuclear pathways of eye movement control (▶Fig. 13.3).
13.3 Understanding Eye Movements
Movements of the eyes are produced by the six extraocular muscles that are innervated by cranial nerves III (oculomotor nerve), IV (trochlear nerve), and VI (abducens nerve). To change visual fixation or to maintain fixation on an object that is moving relative to the observer, the eyes have to move with exquisite precision, and both eyes must move together. This requires a high degree of coordination of both the individual muscles to each eye and the muscle groups in each orbit. To achieve this, the nuclei of cranial nerves III, IV, and VI are controlled as a group by higher centers in the brainstem and the cerebrum.
Eye movements can be classified as follows, based on their role in vision:
1. Those that hold images steady on the retina
● Fixation: holds the image of a stationary object on the fovea when the head is immobile
● Vestibular (vestibulo-ocular reflex [VOR]): holds the image steady on the retina during brief head movements (tested using the oculocephalic reflex)
● Optokinetic: holds the image steady on the retina during sustained head movements
2. Those that direct the fovea to an object of interest
● Saccades: bring the image of an object of interest rapidly onto the fovea
● Smooth pursuit: holds the image of a small moving target on the fovea
● Vergence: moves the eyes in opposite directions (convergence or divergence) so that images of a single object are held simultaneously on both fovea
Six muscles are responsible for eye movements:
● Medial rectus muscle: performs adduction
● Lateral rectus muscle: performs abduction
● Superior and inferior rectus muscles: elevate and depress the eye, respectively, performing these functions best when the eye is abducted.
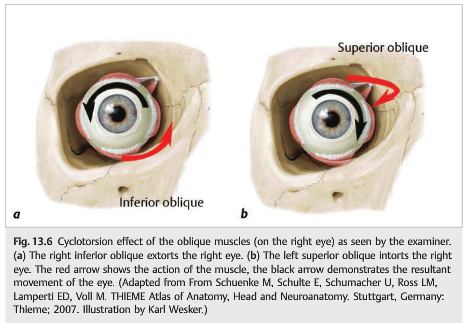
● Superior and inferior oblique muscles: work using a sling/pulley mechanism, with insertions of the muscles being located toward the posterior portion of the globe. The oblique muscles serve as rotators of the eye about the vertical and horizontal axis as the eye is viewed (clockwise or counterclockwise torsion), but also serve to elevate or depress the eye in adduction.
○ Superior oblique muscle: primarily intorts the eye (rotates the superior aspect of the globe toward the nasal bridge about the vertical axis, clockwise in the case of the right eye as viewed by the examiner); this muscle also depresses the eye in adduction.
○ Inferior oblique muscle: extorts the eye but also serves as an elevator in adduction.
In the primary position of gaze, the superior and inferior oblique and superior and inferior rectus muscles all perform a combination of vertical and torsional actions.
13.3.1 Laws of Ocular Motor Control
An agonist muscle moves the eye toward the desired direction. An antagonist muscle moves the eye away from the desired direction. According to Sherrington’s law of reciprocal innervation, whenever an agonist muscle receives an excitatory signal to contract, an equivalent inhibitory signal is sent to the antagonist muscle of the same eye (e.g., in left gaze the right medial rectus is excited while the right lateral rectus is inhibited).Yoke muscle pairs are pairs of muscles (one from each eye) that move both eyes toward the same direction (e.g., the left lateral rectus and the right medial rectus contract simultaneously in leftward gaze). According to Hering’s law of equal innervation, during conjugate eye movements, the muscles in the yoke muscle pair receive equal innervation so that the eyes move together.
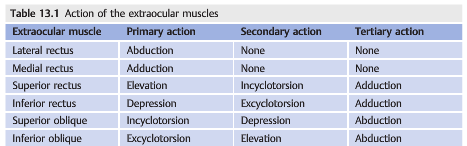
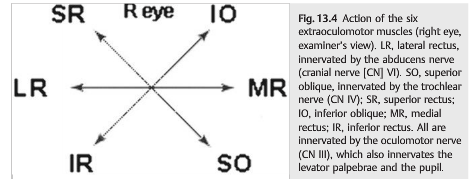
13.3.2 Actions of the Extraocular Muscles
The primary action of an extraocular muscle is its major effect on the eye while the eye is looking straight ahead (in primary position). The secondary and tertiary actions of an extraocular muscle are additional effects on the eye while it is in primary position (▶Table 13.1,▶Fig. 13.4).
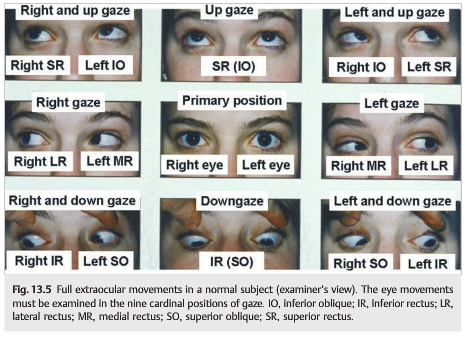
During the clinical examination, the primary position refers to the position when the eyes look straight ahead. The patient is then asked to look right, left, up, and down and then to look up and right, down and right, up and left, and down and left (▶Fig. 13.5).
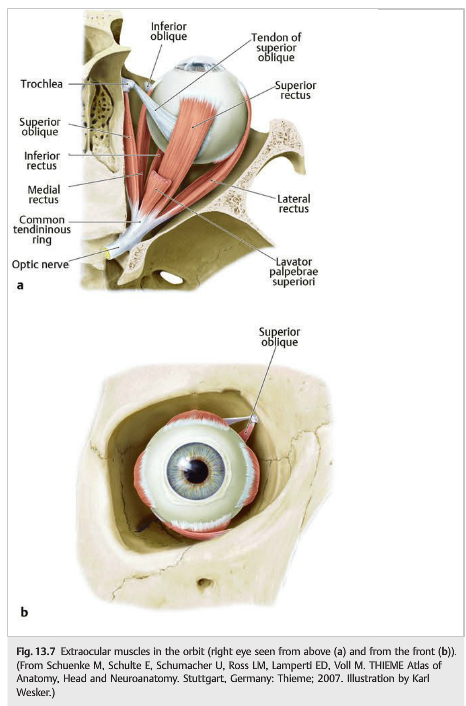
The superior and inferior oblique muscles also rotate the eye, out for the inferior oblique (extorsion) and in for the superior oblique (intorsion) (▶Fig. 13.6, ▶Fig. 13.7, ▶Fig. 13.8).
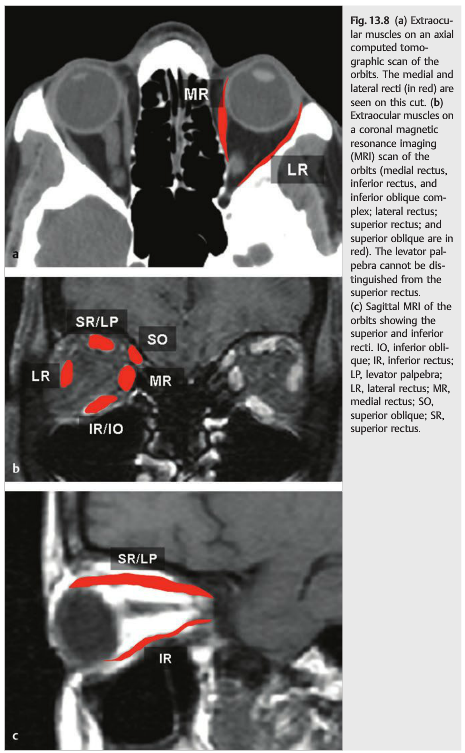
13.3.3 Cranial Nerves
The three ocular motor cranial nerves (III, IV, and VI) innervate the six extraocular muscles of each eye, the major eyelid elevator, and the parasympathetics (for pupillary constriction and lens accommodation) (▶Fig. 13.9).
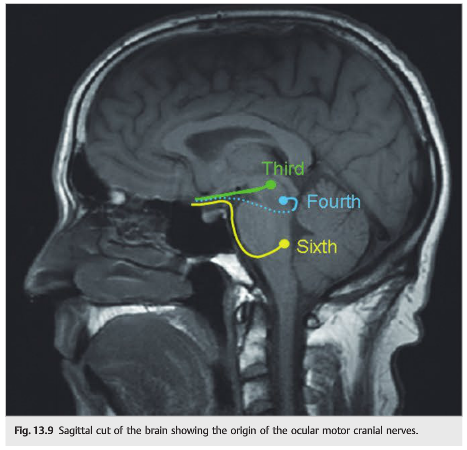
The third cranial nerve (oculomotor nerve) innervates the medial rectus, inferior rectus, superior rectus, inferior oblique, and levator palpebrae muscles, and it provides the parasympathetic pathway (pupillary constriction and accommodation).The fourth cranial nerve (trochlear nerve) innervates the superior oblique muscle. The sixth cranial nerve (abducens nerve) innervates the lateral rectus muscle. All cranial nerves originate in the brainstem, where their nuclei are located. Each nerve has a short course within the brainstem (fascicle) prior to emerging and traveling in the subarachnoid space. Then all ocular motor cranial nerves enter the cavernous sinus and the superior orbital fissure to reach their corresponding extraocular muscles in the orbit. It is essential to understand the anatomical course of each cranial nerve to evaluate a patient with a cranial nerve palsy. By looking at accompanying signs, it is generally possible to accurately localize the lesion (▶Fig. 13.10).
Fig.13.10 Course of the third, fourth, sixth,and fifth cranial nerves(sagittal view). (From Schuenke M, Schulte E,Schumacher U, Ross LM, Lamperti ED, VollM. THIEME Atlas of Anatomy, Head and Neuroanatomy. Stuttgart, Germany:Thieme; 2007. Illustration by Karl Wesker.)
13.3.4 Internuclear and Supranuclear Pathways
The initiation of conjugate eye movements is controlled by pathways and centers above the third, fourth, and sixth nerve nuclei (supranuclear pathways) and by interconnections among these nuclei (internuclear pathways). Inputs from the vestibular system(vestibulo-ocular pathways) also play an important role in the maintenance of eye position with head movement.
13.4 Examination of Eye Movements
Commonly Confused Ocular Motility Terms
Strabismus
This term is commonly used to describe ocular misalignment. It is a nonspecific term that does not indicate the underlying mechanism. It is, however, often used by ophthalmologists to describe congenital ocular deviation (i.e., congenital strabismus) rather than acquired ocular deviations. Neurologists do not use this term.
Comitance/Incomitance
Ocular misalignment (or strabismus) may be comitant or incomitant.
● With comitant (or concomitant) strabismus, the magnitude of ocular deviation is the same in all directions of gaze and does not depend on the eye used for fixation.
● With incomitant (or noncomitant) strabismus, the deviation varies in different directions of gaze. Most incomitant strabismus is caused by a paralytic or a mechanical restrictive process. The deviation is the largest when the eyes turn in the direction of the paralytic muscle. The deviation in incomitant strabismus also varies with the eye used for fixation. When the normal eye is fixating, the amount of misalignment is called the primary deviation. When the paretic eye is fixating, the amount of misalignment is called the secondary deviation. The secondary deviation is larger than the primary deviation in incomitant strabismus because an increase in innervation is needed for a paretic eye to fixate a target. By Hering’s law, the contralateral yoke muscle also receives more innervation, resulting in a larger deviation.
Causes of incomitant misalignment are as follows:
● Extraocular muscle disease
● Myasthenia gravis
● Third, fourth, or sixth nerve palsy
● Internuclear ophthalmoplegia
● One-and-a-half syndrome
Causes of comitant misalignment are as follows:
● Early childhood strabismus
● Loss of fusion (severely decreased vision in one eye)
● Acquired vergence disturbance (convergence, divergence)
● Long-standing sixth nerve palsy (spread of comitance)
● Skew deviation
Phoria/Tropia
A phoria (heterophoria) is an ocular deviation that occurs only when binocular fixation is disturbed, such as when one eye is covered. When viewing an object with both eyes, a subject with a phoria is capable of aligning the eyes to achieve fusion (single binocular vision). The descriptive prefixes (eso-, exo-, hyper-) are used to describe the heterophoria. A tropia (heterotropia) is present even when both eyes are viewing and may result in diplopia. Similarly, the descriptive prefixes (eso-, exo-, hyper-) are used to describe the heterotropia. Although phorias are very common in the general population, a phoria or a tropia has the same localization value in a patient with new-onset binocular diplopia.
Right and Left Designations of Phorias and Tropias
When a horizontal strabismus is incomitant and one eye is obviously deviated, then it makes sense to say “right esotropia” or “right exotropia.” In comitant horizontal strabismus, both eyes contribute equally to the problem, and the side is not designated. However, for vertical deviation, a side must be designated. Generally, the term hypertropia is preferred to hypotropia, and the patient is said to have a “right hypertropia” or a “left hypertropia” depending on which eye is higher. But “right hypertropia” or “left hypotropia” say the same thing: the right eye is higher than the left eye. These terms are describing the position of each eye only as it relates to the other and do not indicate the side of the pathological process. For example, a patient with a left third nerve palsy and an elevation deficit of the left eye may be described as having a “right hypertropia.”
Ocular Motor Nerves/Oculomotor Nerve
Ocular motor nerves refers to all three cranial nerves involved in ocular movements. The oculomotor nerve is cranial nerve III alone.
13.4.1 Assessing Ocular Motility
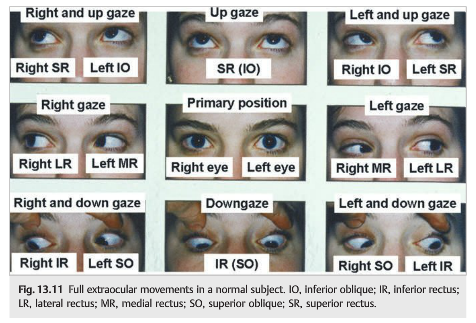
The objective of the motility examination is to evaluate the integrity of the supranuclear and internuclear pathways, ocular motor nuclei, and ocular motor nerves and their muscles. Ductions (monocular eye movements) and versions (conjugate eye movements of both eyes) should be checked in the nine cardinal positions of gaze(“look up, look down, look right, look left”) (▶Fig. 13.11).
The examiner should assess the eye movement by recording it as a percentage of normal.For example, an abduction deficit in an isolated right sixth nerve palsy would be recorded as follows (▶Fig. 13.12):
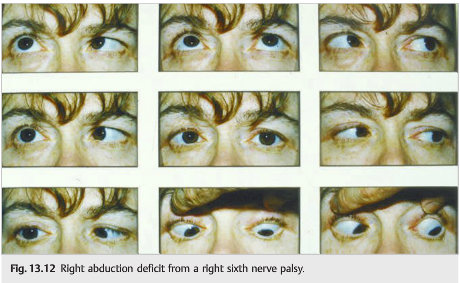
● Incomplete abduction of the right eye (20% of normal)
● Normal elevation, adduction, and depression of the right eye
● Full left eye movements
● Absence of ptosis
● Normal pupils
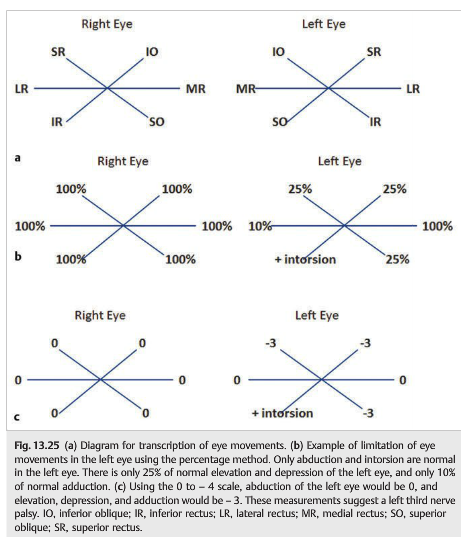
Another way to record eye movements is to use a scale from − 4 to 0 (with − 4 being complete paresis) and 0 being full eye movement (discussed later in chapter, ▶Fig. 13.25c). With this scale, the incomplete abduction deficit shown in ▶Fig. 13.12 would be described as a − 3 abduction of the right eye.
Paresis or Restriction
When movements of one or both eyes are limited, it is important to determine whether the limitation is due to a paresis of the muscle or a restriction of the muscle. For example, an abduction deficit from a sixth nerve palsy results from a paresis of the lateral rectus muscle. On the other hand, an abduction deficit from an enlarged medial rectus in thyroid eye disease results from restriction of the medial rectus. Additionally, an elevation deficit of one eye after an orbital floor fracture is most often due to a restriction of the inferior rectus that is bruised or trapped within the fracture.
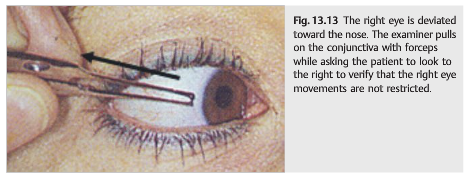
In cooperative patients, the forced duction test allows differentiation between paresis and restriction (▶Fig. 13.13) and is performed as follows:
● Instill two drops of topical anesthetic in the eye.
● Attempt to move the eye by pushing on the deviated globe with a cotton tipped swab or by pulling on the conjunctiva with forceps, while asking the patient to look in that direction.
● Inability of the examiner to move the eye suggests restriction.
Reference:
1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
These questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections totcooper@stanford.edu.