Questions:
1. What should be done immediately when a patient presents with a recent vascular TMVL?
2. What should be done emergently in the presence of an acute central retinal artery or branch retinal artery occlusion?
3. What is the chance and timeline of stroke after TMVL in the presence of ipsilateral atheromatous internal carotid stenosis ≥50%?
4. What is the yearly risk of vascular death (myocardial infarction) in patients with TMVL and atheromatous disease?
 1
1
____________________________________________________
Questions with answers:
1. What should be done immediately when a patient presents with a recent vascular TMVL?
Vascular TMVL is clearly a marker of systemic vascular disease and should prompt an immediate evaluation with the help of a stroke neurologist.
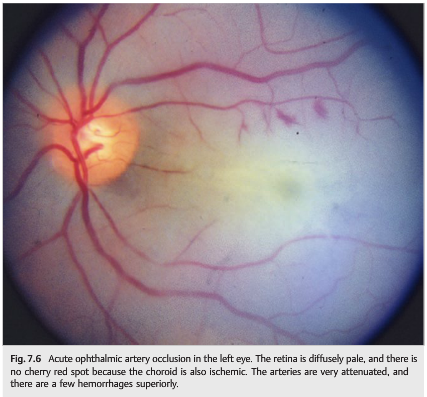
2. What should be done emergently in the presence of an acute central retinal artery or branch retinal artery occlusion?Acute ischemic stroke was detected in 8 (24.2%) subjects with RAO. As with TMVL an immediate evaluation with the help of a stroke neurologist.
3. What is the chance and timeline of stroke after TMVL in the presence of ipsilateral atheromatous internal carotid stenosis ≥50%?
TMVL patients and ipsilateral atheromatous internal carotid stenosis ≥50% have a risk of infarction of 10% at 3 years, the majority of which occurs within a few days after the episode of TMVL.
4. What is the yearly risk of vascular death (myocardial infarction) in patients with TMVL and atheromatous disease?
The risk of vascular death (myocardial infarction) is estimated to be about 4% per year in patients with TMVL and atheromatous disease.
Explanation: “Natural History
The natural history of vascular TMVL varies depending on the age of the patient and on the etiology of the TMVL. Vascular TMVL is clearly a marker of systemic vascular disease and should prompt an immediate evaluation with the help of a stroke neurologist.
Patients with vascular TMVL face a number of risks. Among them are irreversible visual loss (central retinal artery occlusion), which is estimated to be about 1% per year in patients with internal carotid stenosis; and cerebral infarction, whose rate varies depending on the cause of TMVL. TMVL patients and ipsilateral atheromatous internal carotid stenosis≥50% have a risk of infarction of 10% at 3 years, the majority of which occurs within a few days after the episode of TMVL. The risk of cerebral infarction increases with the degree of carotid stenosis. Additionally, the risk of vascular death (myocardial infarction) is estimated to be about 4% per year in patients with TMVL and atheromatous disease.
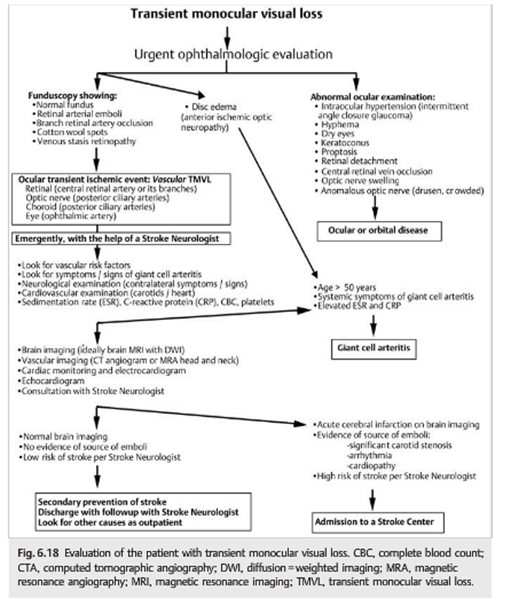
Patient Evaluation The patient evaluation varies depending on the clinical presentation and the patient’s characteristics (▶Fig. 6.18). Patients seen on the day of TMVL should be evaluated emergently, and giant cell arteritis should be ruled out in all patients older than age 50.
Pearls
Intermittent choroidal and optic nerve ischemia may produce TMVL in patients with giant cell arteritis. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) should be obtained systematically in all patients older than age 50 with TMVL.
An ocular examination needs to be performed immediately. If a vascular cause is suspected, blood tests including complete blood count, platelets, ESR, and CRP are obtained emergently.
Pearls
Vascular TMVL is a medical emergency similar to cerebral TIAs. The American Heart Association recommends that patients with presumed vascular TMVL undergo the same immediate workup as those with cerebral TIAs, including brain imaging (ideally brain magnetic resonance imaging [MRI] with diffusion-weighted images). It is common to discover asymptomatic cerebral infarctions on brain MRI of patients with isolated TMVL.”1
Pearls
“The association of branch or central retinal artery occlusion with anterior ischemic optic neuropathy is highly suggestive of giant cell arteritis.”1
Pearls
“Look for giant cell arteritis in the elderly patient with rapidly worsening ocular ischemic syndrome. Giant cell arteritis involves branches of the external carotid artery, which usually supply most of the eye via collateral circulation when there is an internal carotid occlusion. Any disorder affecting branches of the external carotid artery (e.g., giant cell arteritis) will compromise the collateral circulation and may precipitate acute ocular ischemia.”1
Co-occurrence of Acute Retinal Artery Occlusion and Acute Ischemic Stroke-Diffusion-weighted MRI study.
PURPOSE: To evaluate the co-occurrence of acute ischemic stroke and acute retinal artery occlusion (RAO).
DESIGN: Retrospective observational case series.
METHODS: We included 33 consecutive patients with acute RAO who underwent diffusion-weighted magnetic resonance imaging within 7 days of the onset of visual symptoms. The causes of RAO were classified according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria, which are based on clinical features and the results of etiological evaluations for atherosclerosis, cardioembolism and other prothrombotic conditions. We evaluated the prevalence of accompanying acute ischemic stroke in subjects with acute RAO and examined the relationships with etiological parameters.
RESULTS: Acute ischemic stroke was detected in 8 (24.2%) subjects with RAO. Among these subjects, 3 (37.5%) patients did not exhibit any neurologic symptoms or signs. Most of the infarction patterns were small, multiple and scattered. All of the subjects with RAO who were positive for lesions on diffusion-weighted imaging had identifiable causes, whereas only 36% of the subjects who were negative for lesions had identifiable etiologies (P = .003). Carotid stenosis or cardioembolic sources were found more commonly in cases of central retinal artery occlusion (CRAO; 7/18, 38.9%) than in cases of branch retinal artery occlusion (BRAO; 1/15 6.7%, P = .046).
CONCLUSIONS: Acute cerebral infarctions frequently accompany RAO. We recommend diffusion-weighted imaging for patients with RAO because the presence of lesions on diffusion-weighted imaging is accompanied by a significantly increased probability of identifying the cause.2
References:
1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
2. Co-occurrence of Acute Retinal Artery Occlusion and Acute Ischemic Stroke-Diffusion-weighted MRI study. Lee J, et al. AJO. 2014:157(6):1231-1238
More than 600 additional neuro-ophthalmology questions are freely available at http://EyeQuiz.com.
Questions prior to September 2016 are archived at http://ophthalmology.stanford.edu/blog/
After that, questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions, and corrections to tcooper@stanford.edu.