Question: Which of the following are correct for visual evoked responses?
1.Abnormal responses may occur if the patient does not look at the screen, does not focus on the screen, moves the tested eye, or is tired.
2. Appropriate refraction is necessary.
3. The visual evoked response reflects the integrity of the afferent visual pathway (damage anywhere from the retina to the occipital cortex may alter the signal).
4. It is primarily a function of central visual function because such a large region of the occipital cortex near the recording electrodes is devoted to macular projections.
5. Visual evoked responses are not useful in evaluating the integrity of the visual pathway in infants and inarticulate adults.
6. Visual evoked responses cannot provide an estimate of visual acuity when stimuli of various sizes are used.
 1
1
____________________________________________________
Correct Answers:
1. Abnormal responses may occur if the patient does not look at the screen, does not focus on the screen, moves the tested eye, or is tired.
2. Appropriate refraction is necessary.
3. The visual evoked response reflects the integrity of the afferent visual pathway (damage anywhere from the retina to the occipital cortex may alter the signal).
4. It is primarily a function of central visual function because such a large region of the occipital cortex near the recording electrodes is devoted to macular projections.
Explanation: “Visual evoked responses (or visual evoked potentials) are measurements of the electrical signal recorded at the scalp over the occipital cortex in response to visual stimuli. In the test, the patient is asked to look at a TV screen on which various stimuli are provided; electrodes placed on the scalp over the occipital cortex record the responses. Each eye is tested separately
This test is not accurate if the patient does not cooperate. Abnormal responses may occur if the patient does not look at the screen, does not focus on the screen, moves the tested eye, or is tired. Appropriate refraction is necessary.
The visual evoked response reflects the integrity of the afferent visual pathway (damage anywhere from the retina to the occipital cortex may alter the signal). It is primarily a function of central visual function because such a large region of the occipital cortex near the recording electrodes is devoted to macular projections.
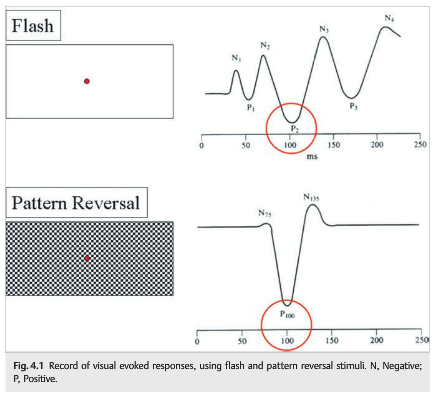
Two techniques are used to record visual evoked responses: pattern stimulus, which provides a quantifiable and reliable waveform but may be absent in patients with poor vision, and flash stimulus, which is useful for patients with very poor vision in whom the pattern stimulus response is absent. The recorded responses for each eye are then compared, with the focus on the amplitude and peak latency of the wave-form (P100). Classically, the P100 waveform is delayed in patients with demyelinating optic neuritis.
In most clinical situations, the visual evoked responses are of limited usefulness and are not necessary to make the diagnosis of optic neuropathy.
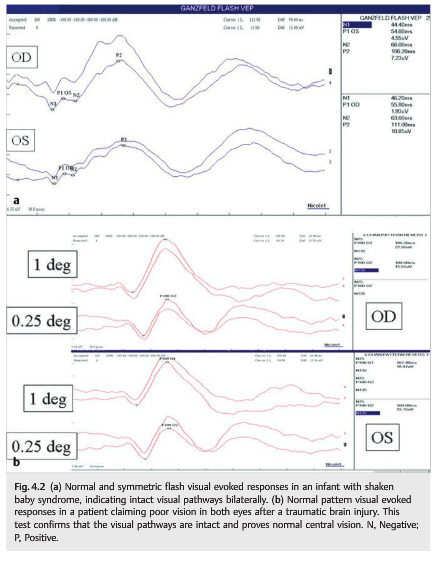
Visual evoked responses are most useful in evaluating the integrity of the visual pathway in infants and inarticulate adults. A preserved flash or pattern response confirms intact pathways, whereas an abnormal flash response indicates gross impairment. An abnormal pattern response is less useful: it may indicate damage, or it may be falsely abnormal.
Visual evoked responses are also useful in confirming intact visual pathways in patients with markedly abnormal subjective visual responses of suspected nonorganic origin. A response with an intact pattern not only confirms intact visual pathways but also provides an estimate of visual acuity when stimuli of various sizes are used. A response with an abnormal or absent pattern does not confirm organic disease because voluntary inattention or defocusing can markedly alter the pattern waveform.”1
 1
1
Reference:
1. Neuro-ophthalmology Illustrated-2nd Edition. Biousse V and Newman NJ. 2012. Theme
More than 600 additional neuro-ophthalmology questions are freely available at http://EyeQuiz.com.
Questions prior to September 2016 are archived at http://ophthalmology.stanford.edu/blog/
After that, questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions and corrections to tcooper@stanford.edu.