Question1:
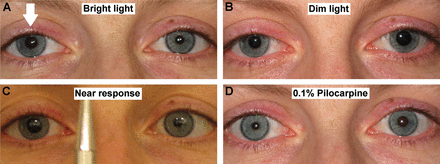
A 35-year-old woman is evaluated for a 2-week history of photophobia and awareness that her right pupil is larger than the left. Examination shows absent right pupillary response to light stimulation of either eye. There is no diplopia and no evidence of extraocular muscle palsy. Upon local instillation of 0.125% pilocarpine, the larger pupil becomes smaller than the contralateral pupil.
Which of the following is the most likely location of the lesion?
1. ciliary ganglion
2. Edinger-Westphal nucleus
3. oculomotor nerve
4. optic chiasm
5. pretectal nucleus
 2
2
__________________________________________
Correct Answer: 1. ciliary ganglion
Explanation:
“This patient has a right Adie tonic pupil. The affected pupil is dilated and poorly reactive to light. Within the first 1 or 2 weeks of its denervation, the iris sphincter will become supersensitive to cholinergic agents such as pilocarpine diluted to a concentration of 0.125% or less. Following 1 drop placed in each eye, a positive response to dilute pilocarpine is either (1) the larger pupil constricts 0.5 mm more than the normal pupil or (2) the larger pupil becomes the smaller pupil. In the absence of associated ptosis or ocular motility deficits, a positive dilute pilocarpine test indicates postganglionic parasympathetic denervation of the iris. In this case, the denervation is likely etiologic, hence a diagnosis of Adie pupil. An isolated unilateral mydriasis as the sole manifestation of an oculomotor nerve palsy is exceedingly rare.”1
Adie Pupil is the most likely diagnosis with the lesion in the ciliary ganglion.
A pupil dilated due to a 3rd nerve palsy will also be supersensitive to pilocarpine 0.125%, however other signs of a 3rd nerve palsy would be present (ptosis, reduced ocular movements, or ocular misalignment).
For more information, refer to page 1011 of the CONTINUUM article “Diagnostic Approach to Pupillary Abnormalities.”
“Adie’s Tonic Pupil, also known as Adie’s Syndrome or Holmes-Adie Syndrome, is a disorder of the autonomic nervous system characterized by mydriasis with poor or sluggish pupillary constriction in bright light with slow redilation and decreased deep tendon reflexes.[1] The entity is named after William John Adie, an Australian neurologist who extensively described the features.[2] When paired with segmental anhidrosis it is termed Ross’ Syndrome.[3]
Etiology
At this time, the underlying etiology of this disease is unknown.
Epidemiology
Adie’s tonic pupil occurs in a 3:1 female to male ratio with an average age of onset of 32 years.[1]
General Pathology
It is thought that either a bacterial or viral infection causes inflammation which damages neurons in the ciliary ganglion of the orbit as well as the dorsal root ganglion in the spinal cord. This damage leads to sectoral denervation of the iris sphincter muscle and poor or sluggish constriction of the pupil in bright light but with normal near response and slow redilation. Roughly 80% of cases are unilateral, but can become bilateral (4% chance per year).[4] Damage to the dorsal root ganglion leads to areflexia. These symptoms do not always occur simultaneously, and the onset of areflexia often occurs after the onset of the tonic pupil.
Pathophysiology
Histologic examination of patients with Adie’s Syndrome has shown a reduction of ciliary ganglion cells.[1] The affected short ciliary neurons are postganglionic parasympathetic neurons which synapse within the ciliary ganglion and innervate the iris sphincter muscles. This denervation leads to sectoral palsy of the iris sphincter muscle, stromal thinning, and occasionally iris atrophy.[1] Over time the neurons regenerate allowing for recovery of the near response. A similar process is felt to occur in the dorsal root ganglion of the spinal cord where pre- and post-ganglionic parasympathetic fibers synapse. These fibers provide parasympathetic innervation to various muscles depending on the reflex involved.
Diagnosis
The diagnosis of Adie’s tonic pupil is clinical, based on history and physical exam.
History
The classic history for Adie’s tonic pupil will be a patient, most commonly a woman in her third or fourth decade of life, with symptoms of blurred vision, photophobia, and anisocoria with difficulty reading.
Physical examination
Examination reveals anisocoria greater in light than dark indicating dysfunction of the parasympathetically innervated iris sphincter muscle in the affected eye. The affected pupil will also slowly constrict and preferentially to a near stimulus than to light. Pupil motility can be further tested by having a patient focus on a near target and one should see normal or near normal pupillary constriction. When then asked to focus on a distant target the affected pupil will slowly dilate when transitioning from near to distance vision when compared to the normal eye. On slit lamp exam, sectoral iris paralysis is appreciated as segmental contracture of the iris sphincter seen as vermiform movements of the pupillary margin. Areflexia is often elicited, especially of the Achilles’ tendon. Areflexia often does not develop at the same time as the tonic pupil and may not be elicited on first presentation.
Signs
Patients will demonstrate anisocoria greater in light than dark with segmental iris palsies. They may also have areflexia, especially of the Achilles’ tendon.
Symptoms
Patients often present with blurry vision often noted especially when transitioning from near to distance vision. Patients also may present with photophobia.[5][6]
Diagnostic procedures
The denervated sphincter muscles can show increased sensitivity to dilute pilocarpine (0.125%) due to up regulation of receptors in about 80% of cases. Dilute pilocarpine can be made by diluting readily available commercial 1% solution with sterile saline. There are studies which show that even normal pupils can react to dilute pilocarpine (0.125%) and that a more dilute solution of 0.0625% or even 0.03125% is more specific for identifying tonic pupils.[7] After 30-60 minutes the affected pupil will constrict more than the normal pupil.
Laboratory test
While the diagnosis of Adie’s tonic pupil is clinical, other causes of tonic pupil must be ruled out. Syphilis serologies should be checked, and a thorough history should be obtained for diabetes, trauma, or other neurological diseases such as Charcot-Marie-Tooth disease or Miller-Fisher syndrome.[8][9]
Differential diagnosis
The differential diagnosis for Adie’s tonic pupil includes trauma, varicella-zoster, giant cell arteritis, tertiary syphilis, Sjögren syndrome, diabetes mellitus, chronic alcoholism, amyloidosis, cancer-associated dysautonomia, Miller-Fisher syndrome, Charcot-Marie-Tooth disease.
Management
General treatment
While in general treatment is not required for Adie’s tonic pupil, dilute pilocarpine can be used for symptomatic relief in cases with severe photophobia.
Prognosis
Adie’s tonic pupil is not a life threatening disease, but can cause photophobia and blurry vision due to poor iris function. With time, ranging from months to years, the affected pupil often constricts with resolution of most symptoms.[1]”2
It is true that a dilated pupil from a 3rd nerve palsy will be supersensitive to 0.1% pilocarpine. However, an eye dilated pupil from a 3rd nerve palsy will always have some ocular motility abnormality.
Abstract:
“Objective: To determine whether the degree of cholinergic supersensitivity of the pupil differs in patients with preganglionic injury of the oculomotor nerve (third nerve palsy) compared with patients with postganglionic injury (Adie’s pupil).
Methods: In this retrospective study, the authors first identified 11 patients with oculomotor nerve palsy and 11 patients with unilateral Adie’s pupil who demonstrated supersensitive pupillary responses using dilute pilocarpine. The same methods for testing supersensitivity of the iris sphincter, and for defining its presence, had been used in both groups of patients. Pupil diameters of the affected and unaffected fellow eye were measured directly from self-developing photographs obtained before and 30 minutes after pilocarpine 0.1% was applied to both eyes. The amount of absolute constriction of the affected pupil, as well as the net constriction of the affected pupil (i.e., the amount of pilocarpine-induced constriction of the unaffected pupil subtracted from the amount of pilocarpine-induced constriction of the affected pupil), was compared between the two groups of patients using the Mann-Whitney test.
Results: No significant differences were identified in any of the comparisons.
Conclusions: The degree of cholinergic supersensitivity of the iris sphincter appears to be similar regardless of whether the site of injury along the parasympathetic pathway of the oculomotor nerve is preganglionic or postganglionic”.3
“Parasympathetic innervation failure causes a relatively dilated pupil that reacts sluggishly to direct light. The major concern, as with ptosis, is a third cranial nerve palsy, especially one caused by an aneurysm.
However, anisocoria is never caused by a third nerve palsy unless there are other signs of a third cranial nerve palsy—ptosis, reduced ocular movements, or ocular misalignment.
A common cause of isolated anisocoria is a viral infection of the ciliary ganglion (Adie’s syndrome), an orbital structure that receives the parasympathetic component of the third cranial nerve.”4
Simulation of vermiform movement of the iris sphincter muscle – Adie’s Pupil.5 https://drive.google.com/open?id=0By3Px03-NjpTZzNnekd3MnVscWM
From: http://www.mrcophth.com/eyeclipartchua/pupils.html
Video Adie Pupil6 https://drive.google.com/open?id=0By3Px03-NjpTRXJOVVVzRFh4UXM
References:
1. Question, answers and explanation are from Continuum Lifelong Learning in Neurology August 2014 – Volume 20 – Issue 4, Neuro-ophthalmology Available at Lane Medical Library – SuNet UserID & Password Required
2. Adie Tonic Pupil. Crowell EC & Feldman BH. EyeWiki AAO. http://eyewiki.org/Adie’s_Tonic_Pupil
3. Comparison of Cholinergic Supersensitivity in Third Nerve Palsy and Adie’s Syndrome. Jacobson D & Vierkant RA. J Neuroophthalmol. 1998;18(3:171-5
4. Anisocoria. The Eyes Have It. University of Michigan Kellogg Eye Center http://www.kellogg.umich.edu/theeyeshaveit/symptoms/anisocoria.html
5. Simulation of vermiform movement of the iris sphincter muscle – Adie’s Pupil. http://www.mrcophth.com/eyeclipartchua/pupils.html
6. Teaching Video NeuroImages: Acute Adie syndrome, Benjamin R. Wakerley, et. al, Neurology September 11, 2012 vol. 79 no. 11 e97 http://www.neurology.org/content/79/11/e97.full?sid=edd94f48-3045-4340-a102-c00b7fd13480
Video available for download: http://www.neurology.org/content/79/11/e97/suppl/DC1
More than 600 additional neuro-ophthalmology questions are freely available at http://EyeQuiz.com.
Questions prior to September 2016 are archived at http://ophthalmology.stanford.edu/blog/
After that, questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions and corrections to tcooper@stanford.edu.