Question: Which of the following are correct?
1. A heterochromia iridis-associated acquired Horner syndrome is usually due to a lesion of the postganglionic neuron (third order).
2. Heterochromia iridis-associated acquired Horner syndrome only occurs in children?
3. In a patient with isolated heterochromia iridis-associated Horner syndrome, the lighter eye is the one with the oculosympathetic paresis.
4. When both Waardenburg and congenital Horner syndromes occur in the same individual the darker iris is the one with the oculosympathetic paresis.
 1
1
___________________________________
Correct Answers: 1, 3, & 4
1. A heterochromia iridis-associated acquired Horner syndrome is usually due to a lesion of the postganglionic neuron (third order).
3. In a patient with isolated heterochromia iridis-associated Horner syndrome, the lighter eye is the one with the oculosympathetic paresis
4. When both Waardenburg and congenital Horner syndromes occur in the same individual the darker iris is the one with the oculosympathetic paresis.
Explanation:
Don’t it make my blue eyes brown: heterochromia and other abnormalities of the iris.2
Although less common, it would appear that cases of acquired Horner’s syndrome in childhood and adult life may occasionally also give rise to iris heterochromia. Laties [28] reported a case of a 29-year-old female who had developed Horner’s syndrome, with associated heterochromia, following the removal of a neurolemmoma when aged 14. Diesenhouse et al subsequently reported two cases of Horner’s syndrome following sympathectomy, which were associated with the development of iris hyperpigmentation. A number of reports in the literature have also indicated the development of iris heterochromia in children who develop Horner’s syndrome as a result of either a cervical ganglioneuroma, [30] neurolemmoma, or neuroblastoma. [32,33 & 31] Again, it is interesting to note that in all cases of heterochromia-associated acquired Horner’s syndrome, the causal lesion was postganglionic in origin. [29]”
Acquired heterochromia with Horner syndrome in two adults.3
“BACKGROUND: Heterochromia iridis, asymmetry of iris pigmentation, has been well described with congenital Horner syndrome. Acquired heterochromia associated with lesions in the ocular sympathetic pathways in adulthood, however, is rare.
METHODS: Two cases are reported in which sympathectomy in adults resulted in ipsilateral Horner syndrome with heterochromia. In each case, pharmacologic testing with cocaine and hydroxyamphetamine was performed.
RESULTS: In both cases, sympathectomy occurred at the level of the second order neuron, but hydroxyamphetamine testing suggested at least partial third order neuron involvement.
CONCLUSION: Acquired heterochromia can occur in adults. The partial response to hydroxyamphetamine in the two cases presented may reflect trans-synaptic degeneration of the postganglionic neuron. A reduction in trophic influences on iris melanocytes may have contributed to the observed heterochromia.”
When the darker eye has the smaller pupil.4

“Waardenburg and congenital Horner syndromes are both recognized causes of congenital hypochromic iris heterochromia. Each has been linked to disruptions in the pathway of tyrosinase induction, thus leading to a deficiency in melanin production of the iris. These syndromes must be considered in the differential diagnosis of a patient presenting with heterochromia iridis. We present the case of a 20-month old boy afflicted with both congenital Horner syndrome and Waardenburg syndrome, type II. In contrast to the more common presentation of congenital Horner syndrome, the affected iris in this case was the darker of the two because of the effects of the concomitant Waardenburg syndrome on the contralateral iris pigmentation. We are unaware of any other cases presenting with both Horner and Waardenburg syndromes and believe that this case serves as an excellent opportunity to briefly review the pathophysiology involved with these disorders.”
The color of the human eye: a review of morphologic correlates and of some conditions that affect iridial pigmentation.5
“Abstract
Iris color can be affected by a variety of ocular disorders. It is suspected that iris color may not remain constant throughout life. These observations have drawn attention to the morphologic correlates of iris color and its regulation. Differences in the iris color of normal eyes are the result of variable amounts of melanin pigment granules within a constant number of melanocytes in the superficial stroma of the iris. These melanocytes seem to reach their genetically determined amount of melanin in early childhood, and their melanin content usually remains constant in adulthood. Diseases such as Horner’s syndrome and Fuchs’ heterochromic iridocyclitis affect iris color, resulting in a decrease of iris pigmentation. Evidence suggests that melanin content of some melanocytes is subject to adrenergic regulation even past childhood. Application of the prostaglandin analogue latanoprost, on the other hand, leads to an increase in iris pigmentation in some patients. Studies with cultured dermal and uveal melanocytes, as well as with uveal melanoma cells, however, show no increase in cell proliferation when treated with latanoprost in vitro. The mechanisms by which latanoprost affects regulation of iris pigmentation requires further investigation.”
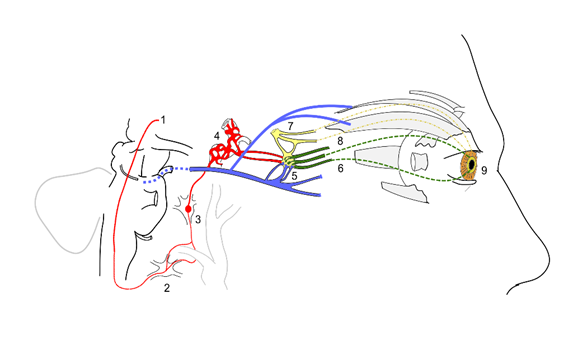
Diagram: Scheme showing sympathetic and parasympathetic innervation of the pupil and sites of lesion in a Horner’s syndrome.6
1. sympathetic fibers arise from the hypothalamus
2. stellate ganglion
3. synapse at the superior cervical ganglion
4. sympathetic plexus around internal carotid artery
5. oculomotor nerve (Cranial nerve 3) fibers synapse at the ciliary ganglion (blue)
6. short ciliary nerves from ciliary ganglion carrying parasympathetic supply to sphincter pupillae (green)
7. trigeminal fibers (Cranial nerve 5) relay in ciliary ganglion and carry sympathetic supply (yellow)
8. long ciliary nerves (from the ophthalmic branch of CN 5) carrying sympathetic supply to the dilator pupillae
9. dilator pupillae muscles of the pupil
Near the stellate ganglion, the sympathetic fibers go around the subclavian artery (shown along with the carotid vessels). This is a site of lesion especially due to its proximity to the apex of the lung (eg. Pancoast’s tumor).
The superior division of oculomotor nerve is shown supplying the superior rectus and levator palpebrae superioris.
References:
1. Orbit/Oculoplastics Quiz 13. Christine A. http://www.djo.harvard.edu/print.php?url=/physicians/kr/769&print=1
2. Don’t it make my blue eyes brown: heterochromia and other abnormalities of the iris. Rennie IG. Eye:2012:26:1:29-50.
3. Acquired heterochromia with Horner syndrome in two adults. Ophthalmology. Diesenhouse MC, Palay DA, Newman NJ, To K, Albert DM. 1992;99(12):1815-7.
4. When the darker eye has the smaller pupil. Wallis DH, Granet DB, Levi L. J AAPOS. 2003 Jun;7(3):215-6.
5. The color of the human eye: a review of morphologic correlates and of some conditions that affect iridial pigmentation. Imesch PD1, Wallow IH, Albert DM. Surv Ophthalmol. 1997;41 Suppl 2:S117-23.
6. Diagram: Scheme showing sympathetic and parasympathetic innervation of the pupil and sites of lesion in a Horner’s syndrome. Autonomic innervation of the pupil and Horner’s syndrome Suraj Rajan commons.wikimedia.org
{kind=link}
More than 600 additional neuro-ophthalmology questions are freely available at http://EyeQuiz.com.
Neuro-ophthalmology Question of the Week prior to September 2016 are archived at http://ophthalmology.stanford.edu/blog/
After that, questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions and corrections to tcooper@stanford.edu.