 4
4
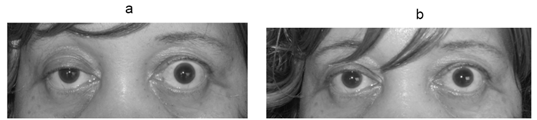
a. Photograph of the patient showing right partial ptosis. The left lid shows compensatory lid retraction because of equal innervation of the levator palpabrae superioris (Herring’s law).
b. Post tensilon test: Note the improvement in ptosis.
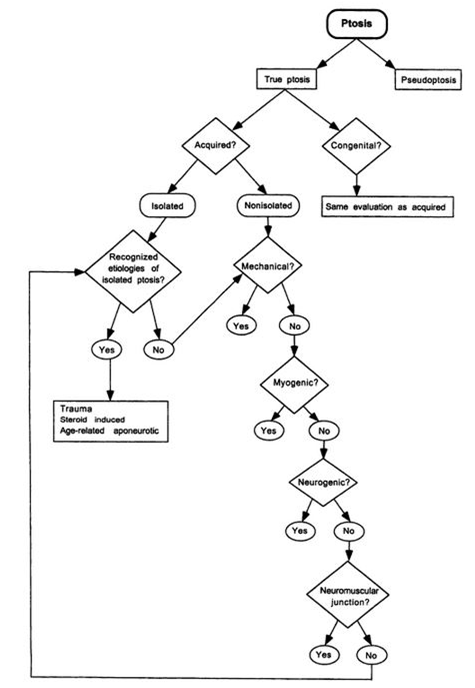
Question: Describe the appropriate steps to take in the emergency department when evaluating ptosis of recent onset.
__________________________________________
ED Concerns – Aneurysm (3rd nerve paresis), Horner syndrome, Myasthenia, Guillian-Barre (Fisher variant), Botulism
ED Ptosis Evaluation
Assess for Pseudoptosis
Apraxia of lid opening (motor neuron, hemispheric and extrapyramidal disease)
Blepharospasm
Hypertropia
● Arrange neuro-ophthalmology appointment
Dermatochalasis
Contralateral lid retraction
Hyperglobus
● Arrange oculoplastics appointment
True Ptosis
Lid deformity = Tumor, infection, chalazion, “lost” but retained contact lens, trauma
● Arrange oculoplastics appointment
No lid deformity
Onset at birth = Congenital ptosis, Myopathies, Jaw-winking phenomenon
● Arrange pediatric ophthalmology appointment
Acquired
Topical steroid use = corticosteroid induced ptosis
● Arrange oculoplastics appointment
No Topical steroid use
Pupillary Abnormality Present
3rd nerve palsy
Horner syndrome
● Arrange emergent MRI of appropriate locations
Guillain Barre (Miller Fisher variant) Pupils may be dilated, without light or near reflex or have tonic reaction.
Botulism
● Neurology consultation
Traumatic iridoplegia
● Arrange ophthalmology clinic follow-up
Pupil Normal
Check Fatigue of Eyelid Elevation, Cogan Lid Twitch & Rest/Ice Pack Test
Positive consider myasthenia gravis
● Order Myasthenia gravis adult antibody screening panel
● Neurology consultation
Negative
Associated neurologic signs
● Brain & Orbit MRI with and without contrast
● Neurology consultation
No associated neurologic signs
Idiopathic “senile” ptosis (levator disinsertion or dehiscence)
● Arrange oculoplastics appointment
From: Clinical Pathways in Neuro-ophthalmology 20032
 3
3
References:
1. Clinical Decisions in Neuro-Ophthalmology, Burde RM, Savino PJ & Trobe JD. 3nd Edition. Mosby 2002
2. Clinical Pathways in Neuro-ophthalmology:An Evidence-Based Approach. Lee AC & Brazis PW. Thieme 2003
3. Cogan’s Lid Twitch Video http://www.kaltura.com/index.php/extwidget/preview/partner_id/797802/uiconf_id/27472092/entry_id/0_u9tn4w8i/embed/auto?
4. Ptosis due to myasthenia with contralateral lid retraction. https://commons.wikimedia.org/wiki/File:Myasthenia_gravis_ptosis_reversal.jpg
{kind=link}
More than 600 additional neuro-ophthalmology questions are freely available at http://EyeQuiz.com.
Questions prior to September 2016 are archived at http://ophthalmology.stanford.edu/blog/
After that, questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions and corrections to tcooper@stanford.edu.