Question: Describe the appropriate steps to take in evaluating sustained monocular vision loss in the emergency department.
 6
6
__________________________________________
ED Concerns: optic neuropathy (giant cell arteritis, pituitary apoplexy, optic nerve compression, typical optic neuritis, atypical optic neuritis, nonarteritic anterior ischemic optic neuropathy), central or branch retinal artery occlusion.
ED Evaluation of Monocular Sustained Vision Loss
1. Rule-out ocular cause
a. Amsler grid and photostress test to rule-out subtle maculopathy
b. Findings of central or branch artery occlusion
– Central artery occlusion – Provide immediate treatment to lower IOP
– Central or branch retinal artery occlusion obtain emergent stroke workup
c. Findings of optic disc edema with a macular star present
– Obtain blood tests for Bartonella henselae and Lyme disease
– Arrange neuro-ophthalmology clinic appointment
d. Evaluate for acute idiopathic blind spot syndrome (AIBSE)3
“All patients were women aged between 19 and 53 years. Twenty-three patients reported positive visual phenomena. Visual acuity was normal in 16 patients. All patients had enlarged blind spots of variable size and density. Dyschromatopsia and afferent pupil defects were prevalent. Ophthalmoscopic features included uveitis, mild optic nerve swelling, granularity of macular pigment, subretinal white dots, and peripapillary pigment disturbances. Twelve of the 13 patients who underwent fluorescein angiography had optic disc staining and 5 had retinal pigment epithelial lesions with late staining. Full-field electroretinogram results were normal in 8 of 9 patients, although focal electroretinogram results were abnormal in 8 of 9 patients. Photopsia always decreased but visual fields did not improve. Six patients experienced recurrence.”3
– Arrange neuro-ophthalmology clinic appointment
2. Assess for optic neuropathy (Decreased acuity, color vision and RAPD)
a. Over age 50 rule-out arteritic anterior ischemic optic neuropathy – Stat CRP, ESR, CBC with platelet count.
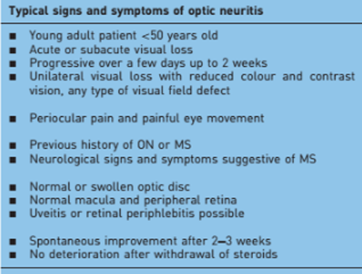
b. Under age 40 assess for typical optic neuritis
– Typical optic neuritis – workup and treat
 5
5
c. Order emergent Brain/Orbit MRI to rule-out optic lesions consistent with MS, compressive optic neuropathy or pituitary apoplexy.
– Abnormal – arrange appropriate emergent consultation
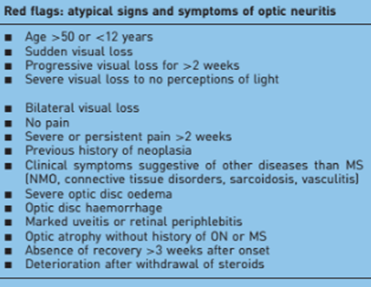
d. If pituitary apoplexy, a compressive lesion or no lesion consistent with MS are present on MRI, consider atypical optic neuritis, toxic, nutritional, hereditary, radiation and nonarteritic anterior ischemic optic neuropathies.
– Atypical Optic Neuritis
 5
5
– Rule-out other potential causes: optic neuropathy.
– Obtain blood tests: syphilis, Lyme disease, Bartonella henselae, HIV, Aquaporin 4 & NMO-Ig, antinuclear antibodies (ANA), anti-double-stranded DNA antibodies, protoplasmic/cytoplasmic antineutrophil cytoplasmic antibodies (p/c ANCA), extractable nuclear antigens (ENA), angiotensin converting enzyme (ACE), interleukin-2 receptor, antiphospholipid Ab, rheumatoid factor, calcium and vitamin B12.
– Obtain neurology consultation for lumbar puncture: opening pressure and total protein, albumin, IgG, IgA, IgM, glucose, lactate, cell count, microbiological and virological analysis and oligoclonal bands.
– Consider chest X-ray and CT scan for sarcoidosis
– Toxic, nutritional, hereditary and radiation causes. Confirm history specific questions to rule out toxin exposure, nutrition deficit including prior gastrointestinal surgery, hereditary optic neuropathy, and radiation exposure and obtain indicated test and arrange consultations.
– After ruling out previous conditions and the patient is over age 40 consider nonarteritic anterior ischemic optic neuropathy.
“Nonarteritic anterior ischaemic optic neuropathy (NAION) is the most common acute optic neuropathy in patients over the age of 50 and is the second most common cause of permanent optic nerve-related visual loss in adults after glaucoma. Patients typically present with acute, painless, unilateral loss of vision associated with a variable visual field defect, a relative afferent pupillary defect, a swollen, hyperaemic optic disc, and one or more flame-shaped peripapillary retinal haemorrhages. The pathogenesis of this condition is unknown, but it occurs primarily in patients with structurally small optic discs that have little or no cup and a variety of underlying vascular disorders that may or may not be known at the time of visual loss. There is no consistently beneficial medical or surgical treatment for the condition, but there are now animal models that allow testing of various potential therapies. About 40% of patients experience spontaneous improvement in visual acuity. Patients in whom NAION occurs in one eye have a 15-19% risk of developing a similar event in the opposite eye over the subsequent 5 years.”4
3. Arrange neuro-ophthalmology clinic for additional evaluation and follow-up.
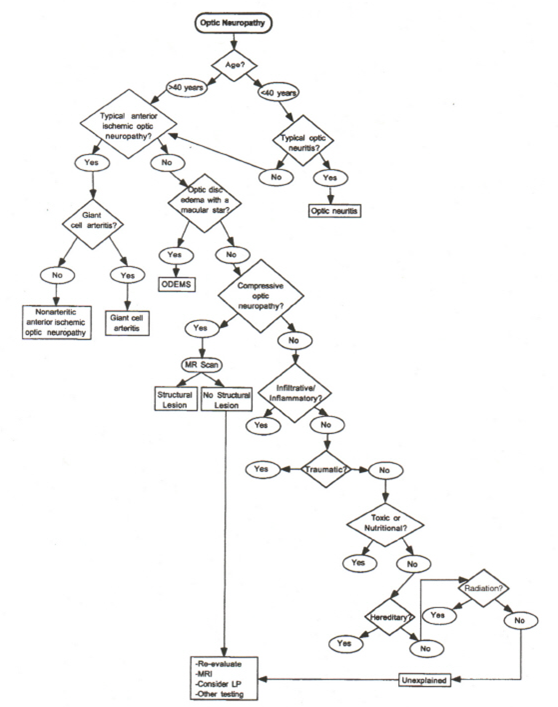
Optic Neuropathy Care Path
From: Clinical Pathways in Neuro-ophthalmology 2003
References:
1. Clinical Decisions in Neuro-Ophthalmology,Burde RM, Savino PJ & Trobe JD. 3nd Edition. Mosby 2002
2. Clinical Pathways in Neuro-ophthalmology:An Evidence-Based Approach. Lee AC & Brazis PW. Thieme 2003
3. Acute idiopathic blind spot enlargement syndrome: a review of 27 new cases. Volpe ND, Rizzo JF, Lessell S. Archives of ophthalmology. 2001:119:1:59-63
4. Current concepts in the diagnosis, pathogenesis and management of nonarteritic anterior ischaemic optic neuropathy. Miller NR & Arnold AC. Eye (Lond). 2015;29(1):65-79.
5. Clinical approach to optic neuritis: pitfalls, red flags and differential diagnosis. Voss E, Raab P & Stangel M. Ther Adv Neurol Disord. Mar 2011; 4(2): 123–134.
6. Branch Retinal Artery Occlusion. Nathan NR, Medscape http://emedicine.medscape.com/article/1223362-overview?src=refgatesrc1
More than 600 additional neuro-ophthalmology questions are freely available at http://EyeQuiz.com.
Questions prior to September 2016 are archived at http://ophthalmology.stanford.edu/blog/
After that, questions are archived at https://neuro-ophthalmology.stanford.edu
Follow https://twitter.com/NeuroOphthQandA to be notified of new neuro-ophthalmology questions of the week.
Please send feedback, questions and corrections to tcooper@stanford.edu.